Diving Safety
Increasing The Probability Of Surviving Loss Of Consciousness Underwater When Using A Rebreather
With divers soon returning to the loop, the Rebreather Training Council (RTC) is currently considering a number of initiatives to improve rebreather diving safety. One of those is to recommend the use of mouthpiece retaining straps to prevent drowning in the event of loss of consciousness (LoC). Accordingly, we offer this seminal paper by ex-British Special Forces dive instructor turned tech instructor trainer Paul Haynes on their efficacy and use. Can you or your mates survive a LoC underwater?

by Paul Haynes. Header image: Deep wreck diver Gareth O’Neill giving scale to one of the impressive 13.5″ gun barrels on the wreck of the King George V-class dreadnought battleship HMS Audacious, which lies in 64m (210 ft.) off the coast of North Donegal, Ireland. Photo by Barry McGill.
Mouthpiece Retaining Strap Resources:
Where do Agencies and Manufactures Stand on Mouthpiece Restraining Straps?
A Mouthpiece Restraining Strap Just Might Save Your Life
We surveyed CCR divers from around the world. Here are the results.
The paper was first published in the Diving and Hyperbaric Medicine Volume 46 No. 4 December 2016 253
When compared to open circuit scuba, it is acknowledged within sport, military and occupational diving organisations that the probability of exposure to an inappropriate breathing gas is increased when using rebreathers. 1
As a result, a serious or fatal incident is more likely when rebreather diving. 2
Inappropriate breathing gas scenarios most frequently associated with rebreather use are: (1) hypoxia; resulting from respiring an hypoxic gas, (2) hypercapnia, resulting from increased levels of inspired carbon dioxide (CO2), or hypoventilation, (3) hyperoxia, resulting from respiring an hyperoxic gas. 3
The sport diving community, defined here as manufacturers, diver training agencies, instructional cadre, and divers, frequently refers to these maladies as the rebreather ‘3H hazards’, all of which can lead to loss of consciousness (LoC) with little or no warning.
The most common interface between the rebreather and the diver’s respiratory system is a mouthpiece valve assembly, frequently called a dive surface valve. This human-machine interface is referred to in this paper as a “mouthpiece” and is used in conjunction with a sport diving “half-mask.” The mouthpiece typically requires manual operation by the diver to change from “surface mode,” which isolates the rebreather re-circulation system (breathing loop) from the environment, to ‘dive mode’, which allows access to the breathing loop and breathing gas.

As tone is lost from the mandibular muscles following LoC, the likely consequence is loss of airway protection as the mouthpiece/breathing loop falls from the mouth of the diver. If this occurs underwater, unless there is immediate intervention by a diving partner, the following outcomes are highly likely: (1) fluid aspiration and asphyxiation, (2) venting of breathing loop gas via the open mouthpiece, (3) whole or partial flooding of the breathing loop, (4) loss of buoyancy, (5) drowning.
Although other factors (triggers) are inevitably responsible for initiating the accident, loss of airway protection and subsequent drowning is most frequently the actual cause of death (CoD). This paper examines a potential means of delaying or limiting this cycle, thus increasing the probability of surviving LoC underwater when using a rebreather.
Background
The mid-1990s saw the beginning of an upsurge in the use of rebreathers by sports divers. At that time, the sport diving industry had limited rebreather experience and so in anticipation of a growth in rebreather popularity, in 1996 the diving industry organised Rebreather Forum Two (RF2). The conference was organised to address the major issues involved in bringing rebreather technology to the consumer market-place and was divided into working sessions to identify the key technology, safety, training, and risk management issues. Drawing on the collective experience of numerous delegates from sport, military, and occupation diving backgrounds, a consensus was developed in order to help shape future sport rebreather diving practice.4
Rebreather Fatality Analysis
As anticipated, sport rebreather use increased post RF2. Subsequently, with consideration to the relatively low number of rebreather sport divers, there appeared to be a disproportionately higher number of reported rebreather fatalities when compared to open-circuit scuba. As a consequence, Divers Alert Network (DAN) conducted a study comparing sport diving open circuit and rebreather scuba fatalities from the period 1998 to 2006.5 Due to the difficulty in attaining comprehensive rebreather accident data specific to each fatality, in particular CoD as determined by a Medical Examiner (Coroner), the DAN study was restricted to a low number of rebreather fatalities (80 cases). However, study conclusions appeared to support the following related 1996 RF2 consensus points:
“Rebreathers are much more complex than open circuit with insidious risk.”
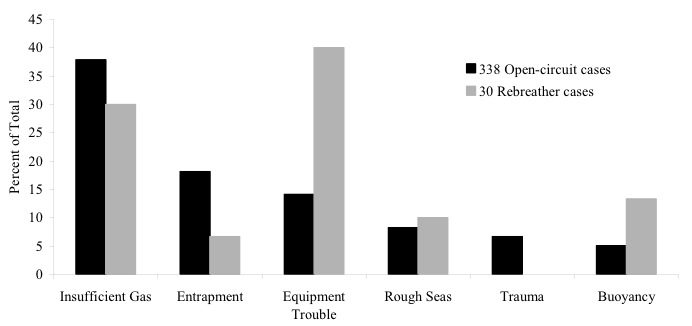
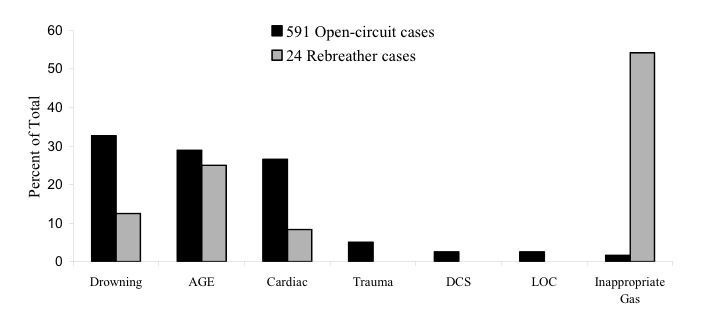
The 2007 DAN analysis concluded that, of the cases studied, equipment trouble (human error or technical failure) was the trigger (something that turns an uneventful dive into an emergency) in over 40% of rebreather fatalities compared to just over 15% of open circuit fatalities (Figure 1). In addition, inappropriate breathing gas (insidious risk) was the disabling injury (something that causes death or makes drowning likely) in over 50% of rebreather cases compared to less than 5% of open circuit cases (Figure 2).
“Loss of consciousness presents a significant hazard when using rebreathers, likely to result in death by drowning.”
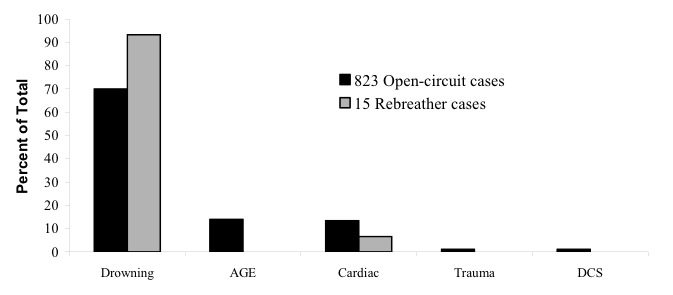
The 2007 DAN analysis concluded that in 94% of cases studied, the actual CoD, as determined by a Medical Examiner, was drowning (Figure 3).
In an effort to quantify rebreather diving risk, in 2013, a separate rebreather fatality study concluded that of the 181 cases analysed between 1998 – 2010, study data suggested a four- to ten-fold increased risk of death when rebreather diving compared to open circuit scuba diving2. The study also reported that a rebreather potentially has a 25-fold increased risk of component failure compared to an open circuit manifolded twin-cylinder scuba system. This study therefore also appears to further support the RF2 consensus statements discussed above.
















Human error
An incident is defined here as an unplanned event that degrades safety and culminates in equipment damage, diver injury, or death. Rebreathers are complex equipment that form one element of a broader life support system that includes: (1) the diver (attitude, skill set, knowledge, experience, health and fitness to dive), (2) dive partner / team (attitude, skill set, knowledge, experience, health and fitness to dive), (3) surface support team (attitude, skill set, knowledge, experience, emergency response protocols, emergency medical facilities), (4) diving ancillary equipment (functionality and fitness for purpose), (5) environmental protection equipment (functionality and fitness for purpose), (6) procedural/diving methodology (appropriateness and fitness for purpose).
Rebreather incident data suggests that a frequent contributing factor is knowingly or unknowingly violating diving and/or equipment protocols as opposed to equipment malfunction.2 This is in keeping with data from the marine oil and gas industry where approximately 80% of incidents investigated were related to human unreliability, and approximately 20% were related to technical causes.6 These figures support a widely held perception amongst the sport rebreather community that the diver is the “weak link” in the life support system “chain” described above.
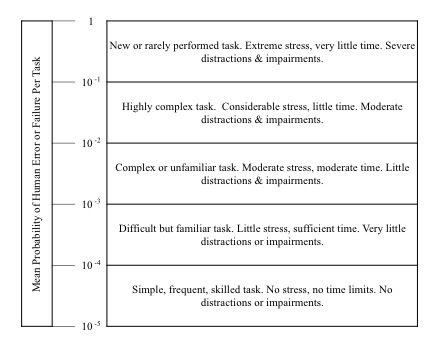
To assist in the estimation and qualification of human error, Swain and Guttman developed a generic rate from experiment and simulation in the operation of nuclear power plants (Figure 4).7 If we consider an experienced rebreather diver in a benign environment, the assembly, testing, pre-dive donning and functionality confirmation (pre-breathe) procedures, all of which are essential to safe rebreather use, could be considered to fall into the fourth row of Figure 4, i.e., difficult but familiar task, little stress, sufficient time, very little distractions or impairments. The mean probability of human error or failure per task for such a scenario is between one in 1,000 events to one in 10,000 events. Thus, even under relatively benign conditions, experienced divers will occasionally make errors. It may be concluded, therefore, that to a lesser or greater extent, all levels of rebreather diver from novice to expert are prone to human error, the consequence of which could be exposure to an inappropriate breathing gas and LoC underwater.
Rebreather Accident Prevention
To help prevent rebreather diving accidents the following key measures are presently implemented or recommended by sport diving training agencies and equipment manufacturers:
- Use of equipment that has been subject to independent third party testing against a recognised international standard
- Appropriate training standards and their strict application by diving instructors
- Appropriate dive planning
- Analysis and clear labelling of all gas cylinders
- Use of assembly and test checklists
- Remaining within manufacturer’s recommendation / performance guidelines
- Remaining within training qualification parameters
- Pre-breathe and function check prior to entering the water
- Diving in pairs/teams
- Frequent oxygen partial pressure display monitoring
- Remaining within appropriate dive planning parameters
- Application of appropriate preventive and corrective maintenance
These incident mitigation measures are also applied within military and occupational diving environments, often to a greater level of detail and enforcement.8, 9 However, despite what is often the rigorous application of equipment maintenance schedules, prescriptive diver supervision, and organisational management systems, in the author’s experience, human error remains a common characteristic of military and occupational rebreather diving incidents. Therefore, within the sport diving environment, it is reasonable to assume that, as a consequence of less formal diving equipment maintenance schedules, supervision, and management practices, human error will likely continue to remain a common characteristic of sport rebreather diving incidents with the resulting potential for LoC.
Airway Protection
Aspiration of as little as 1–3 ml∙kg-1 [0.02-0.05 oz/Ibs] per body weight of water produces profound alterations in human pulmonary gas exchange.10 It is also reported that average water aspiration in drowning is relatively small, rarely exceeding approximately 2.2 ml∙kg-1 [0.03 oz/Ibs] per body weight.11
Therefore, preventing or limiting fluid aspiration following LoC underwater is critical to surviving such an event. Whilst it is acknowledged that the diver may eventually die as a consequence of exposure to an inappropriate breathing gas, this can take a number of minutes or longer depending upon the breathing gas composition and ambient pressure (depth). If water aspiration is prevented or delayed following LoC, a diving partner may be able to affect a successful rescue. Alternatively it is conceivable that under certain circumstances, the distressed diver may regain consciousness, potentially enabling self-rescue.
To mitigate fluid aspiration following LoC underwater, a 1996 RF2 consensus statement endorsed the use of the full-face mask (FFM). However, a FFM adds to equipment complexity, and restricts access to alternative breathing gas supply systems whilst increasing maintenance, training requirements and associated cost. These factors likely account for the sport rebreather diving community having not embraced the widespread use of FFMs despite their potential safety benefits.
One occupational diving equipment manufacturer has developed an innovative hybrid FFM/half mask design.12 This mask system enables the ready separation of the lower oral section of the mask, which incorporates the rebreather mouthpiece. This design offers FFM airway protection benefits whilst also facilitating ready access to alternative breathing gas delivery systems. However, the sale of this hybrid design has generally been confined to government and occupational diving organisations. This and the relatively high cost appear to have restricted its wider use by sport rebreather divers.

In recognition of the possibility of encountering inappropriate breathing gas and the associated potential for LoC underwater, when a FFM is not used, the mouthpiece retaining strap (MRS), combined with related training, has been employed by militaries worldwide for over half a century. It is a common safety design feature of the vast majority of both classic and contemporary military rebreather designs where the manufacturer has endeavoured to provide airway protection in the event of LoC underwater. In its simplest form the MRS is an elasticated adjustable strap secured to the breathing loop/mouthpiece. To optimise its effectiveness, the MRS is worn over the crown of the head and adjusted to positively hold the mouthpiece in position without causing undue discomfort. More sophisticated versions incorporate a padded flange. When retracted around the face by the distended strap, the padded flange enhances the lip seal whilst also helping to secure the mouthpiece in position (Figure 5). The MRS is a relatively low cost, simple and available alternative to the FFM.
Mouthpiece Retaining Strap Efficacy
A literature search has failed to identify any formal evaluation of MRS efficacy. The subject was discussed at Rebreather Forum Three (RF3), Orlando, Florida, in May 2012, and a RF3 consensus statement reads: “The forum identifies as a research question the issue of whether a mouthpiece retaining strap would provide protection of the airway in an unconscious rebreather diver.”13 However, it is unlikely that a meaningful prospective experimental evaluation of the MRS could be undertaken in human subjects. In the absence of a specific formal study, the suggestion of MRS efficacy is principally based upon observational (anecdotal) evidence from military diving sources.
As a measure of the perceived potential effectiveness of the oral seal achieved by a correctly worn MRS, when conducting a diver rescue, some closed circuit oxygen rebreather military user groups are trained to break the MRS oral seal by partially inserting a finger under the unconscious diver’s lip at the corner of the mouth. This is believed to help facilitate the venting of expanding gas from the distressed diver’s lungs and reduce the risk of pulmonary barotrauma on ascent.14 Military groups who train this technique believe that an appropriately designed MRS results in an effective seal between mouth and breathing loop mouthpiece. Anecdotal evidence from various experienced military rebreather divers/diving supervisors, including the author, suggest that the use of a MRS has on various occasions been a key contributory factor to surviving LoC underwater. It is also the author’s experience as a passenger in a free-flooding combat submersible swimmer delivery vehicle, that whilst in an upright fetal position, the MRS has provided airway protection during periods of sleep lasting up to 10 minutes.
These perceptions are corroborated by one notable study that analysed 153 accidents amongst French military rebreather divers.15 Fifty-four of these events led to LoC underwater; however, this resulted in drowning in only three cases. The military report states: “gas toxicities are frequently encountered by French military divers using rebreathers, but the very low incidence of fatalities in over 30 years can be explained by the strict application of safety diving procedures.” These procedures include:
“Systematic linking of divers in pairs, so that a diver can find his buddy regardless of diving conditions (particularly if visibility is poor) and can lend assistance in the event of rescue”.
“Using a strap to hold the mouthpiece in position, along with a lip guard, so that an unconscious diver can still breathe without risk of drowning. The rescuer can then concentrate on the quality of assistance and respecting the diving parameters for regaining the surface”.
The report gives no weighting to either of these factors, so it is unclear which, if any, played a larger role in preventing drowning in 51 out of the 54 LoC events. However, protecting the airway from water aspiration and effecting rescue at the earliest opportunity are cited as key factors to surviving LoC underwater. The related benefit implied by this military diving study is likely to be translatable to the sport diving setting.
Rebreather Solo Diving?
Of the 80 rebreather fatalities reviewed in the 2007 DAN study, 33% (26 cases) involved solo diving as a result of either deliberately diving alone or becoming separated from a diving partner. In support of this finding, whilst its accuracy cannot be readily verified, a publically available on-line collation of sport rebreather fatalities suggests that solo diving continues to remain a prominent characteristic of sport rebreather deaths that have occurred since 2007.16 Due to the increased probability of respiring an inappropriate breathing gas when using a rebreather and the absence of a dive partner to witness early signs of diver distress or performance impairment and to implement rescue, solo rebreather diving appears to present additional risk.

Even a well-designed and correctly fitted MRS is unlikely to provide airway protection over an extended period following LoC. Therefore, to realise any safety benefit accruing from delaying or preventing drowning, the maintenance of close contact with a dive partner is also considered an important component to surviving LoC underwater. This proposition appears to be supported by the French military study, in which divers have survived LoC as a result of MRS use and early rescue by a dive partner.
Sport Rebreather Design And Performance Standards
European standard EN14143:2013 sets minimum design and performance parameters for sport rebreathers sold within the European Union, where compliance is a mandatory aspect of consumer law.17 It is also setting a broader global benchmark for rebreather design standards. However, human error and equipment failure will likely remain a characteristic of sport rebreather use. It follows that the provision of airway protection is a desirable safety design feature regardless of rebreather performance and reliability. Indeed, EN14143:2013 specifies a design requirement regarding a ‘face-piece’, which the standard defines as: “a mouthpiece assembly, a half mask, a full-face mask or a helmet”. The standard goes on to state: “The face-piece shall aid ear clearing by allowing the diver’s nasal passages to be occluded. It shall also minimise the ingress of water during normal use and in the event of a diver falling unconscious or having a convulsion.”
Whilst it is not specified how the minimisation of water ingress is to be implemented, EN14143:2013 states: “The face-piece harness shall be designed so that the face-piece can be donned and removed easily. It shall be adjustable or self-adjusting and shall hold the face-piece assembly firmly and comfortably in position.” The standard subsequently defines the design and functional requirements of a retaining strap, if fitted.
The European rebreather standard therefore recognises the potential safety benefit of protecting the airway and breathing loop in the event of LoC and as a consequence incorporated the requirement into its design specification (Anthony G, personal communication, 2014; principal author of ENI4143:2013).
Market Trends
To extend the exploration parameters of self-contained sport and scientific diving to date, relatively small groups of “technical divers” have been the most prevalent users of rebreathers. However, a considerably larger sales potential is thought to exist amongst mainstream sport divers. As a consequence, considerable resource is presently being applied by the sport diving industry to introduce rebreathers into this larger market place.18, 19
To help facilitate mainstream rebreather diving, the world’s largest recreational diving training agency has defined a generic recreational closed circuit rebreather (rCCR) specification and developed what it considers to be appropriate rCCR training standards. As a consequence, manufacturers are either producing dedicated rCCR models or adapting previous rebreather designs to comply with this rCCR specification.20, 21 Rebreather use will likely continue to increase amongst sport divers.

A mandatory rCCR specification safety feature is the bail out valve (BOV) (Figure 6). In an emergency, it enables the diver to manually access a source of open-circuit breathing gas without the need to remove the mouthpiece. However, it is worth noting that the MRS is not a mandatory rCCR safety feature. Despite the EN14143:2013 design requirement previously discussed, the reason for this remains unclear but may result from the fact that the MRS has historically not formed part of sport rebreather design. Therefore, awareness and experience of its application and potential safety benefit is limited amongst the sport rebreather community. In addition, whereas a BOV is increasingly an integral part of sport rebreather design, contrary to EN14143:2013, it continues to remain the norm for the vast majority of manufacturers to sell sport rebreathers without “a means to minimise the ingress of water in the event of a diver falling unconscious” or a means to “hold the face-piece assembly firmly and comfortably in position.”17
Airway Protection Spectrum
We may consider the upper end of the airway protection safety ‘spectrum’ is an occupational diving helmet interfaced with a rebreather. An example is the Secondary Life Support saturation diving emergency bailout rebreather manufactured by Divex.22 Assuming the watertight integrity of the breathing loop and helmet, water aspiration and, therefore, drowning following LoC, is highly improbable. At the low end of this ‘spectrum’ is the absence of any means of protecting the airway following LoC. Despite acknowledging the increased potential for exposure to an inappropriate breathing gas and LoC when rebreather diving, the sport diving community largely remains posiioned at the low end of this “spectrum.”

Conclusions
Rebreathers incorporate a high number of inherent failure modes and the potential for human error. Individually or in combination this can lead to inappropriate breathing gas and spontaneous LoC underwater. If the airway is unprotected, water aspiration and asphyxiation is the likely immediate outcome. Whilst FFMs are considered to offer a high level of airway protection, due to cost and complexity they are unlikely to be widely adopted by sport rebreather divers.
Military rebreather manufacturers consider the MRS a safety-critical design feature, which is extensively employed throughout the global military rebreather diving community. Observational evidence suggests the correct use of a MRS can be an effective means of preventing or limiting water aspiration immediately following LoC. This potentially extends the window of opportunity for effective rescue or conceivably, self-rescue should consciousness be regained.
In the vast majority of sport rebreather fatalities, drowning is the actual cause of death. Therefore to directly mitigate the immediate consequences of loss of airway protection following LoC underwater, an effective MRS should be a standard component of all rebreathers used by sport divers. In addition, in order to raise awareness of the potential safety benefits, its use should be mandated within sport rebreather training standards.
References
3. Doolette DJ, Mitchell SJ. Hyperbaric conditions.Comprehensive Physiol. 2011;1:163-201.
4. Richardson D, Menduno M, editors. Rebreather Forum2 Proceedings. Redondo Beach, CA: Diving Science and Technology; 1996.
5. Vann RD, Pollock NW, Denoble MD. Rebreather fatality investigation. In: Pollock NW, Godfrey JM, editors. Diving for science 2007. Proceedings of the American Academy of Underwater Sciences 26th Symposium. Dauphin Island, AL: AAUS; 2007.
6. Bea RG, Roberts KH. Human and organisational factors in design, construction and operations of offshore platforms. Offshore Technology Conference. Houston, TX. 1995.
8. US Navy Diving Manual, rev 6. Vol 4. Washington, DC: Department of the Navy; 2008.
12. Kirby Morgan.com [internet]. Santa Barbara, CA. [cited 2016 August 1].
14. Royal Australian Navy Diving Manual. ABR 155. 2005 Vol2. Rev 2. Ch 12. Para 12-70.
15. Gempp E, Louge P, Blatteau JE, Hugon M. Descriptive epidemiology of 153 diving injuries with rebreathers among French military divers from 1979 to 2009. Mil Med. 2011;176:446-50.
17. European standard EN14143: 2013. Respiratory equipment- self-contained re-breathing diving apparatus. European Committee for Standardisation. Para 5.10. 2013.
20. Menduno M. The future of diving. Diver Magazine. 2011;37(3):18-25.
21. Menduno M. Rise of the recreational rebreather. Diver Magazine. 2011;38(8):18-25.
22. Jfdglobal.com [internet] JFD / Divex commercial rebreathers. [cited 2016 August 1].
Dive Deeper:
InDepth: Can Mouthpiece Retaining Straps Improve Rebreather Diving Safety?
InDepth: A Mouthpiece Restraining Strap Might Just Save Your Life
InDepth: RTC Launches New Rebreather Safety Initiative

Paul Haynes is a former UK Special Forces (SF), Special Boat Service (SBS) Combatant Diver Instructor, Diving Supervisor and Swimmer Delivery Vehicle (SDV) Operator. Upon leaving UKSF, he worked for Divex Ltd (now JFD) the world’s largest manufacturer of professional diving equipment. As a result, Paul has remained at the forefront of defense underwater life support systems research, development, design, test and training for over two decades.
Paul is a RAID advanced mixed gas diving and rebreather Instructor Trainer, as well as a PSAI and BSAC instructor, and has authored several rebreather training manuals and numerous safety related articles for civilian diving publications. He has been an invited keynote speaker at numerous technical diving conferences to discuss rebreather development, safety and training, and has provided civilian rebreather accident investigation assistance to U.S. law enforcement. He provides consulting services through his firm Haynes Marine Ltd.
Paul is a prolific shipwreck explorer and has participated in the discovery of numerous deep shipwrecks in the North Sea off the East coast of Scotland, and is a member of the Explorers Club of New York. In addition, he has been the diving safety officer on a number of high profile diving expeditions including UK Ministry of Defence sanctioned 2016 survey of HMS Hampshire, and the joint UK Royal Navy/civilian expedition to recover of the bell from the Battleship HMS Prince of Wales sunk during WWII in the South China Sea.




























Dial In Your DCS Risk with the Thalmann Algorithm

Deep Tunnel Workers Go Trimix

La Grande Dérive

California Dreamin’

British Invasion—Thailand Karst Edition 2024

Harnessing the Power of ‘Educated’ AI to Improve Diving Safety
