Education
Decompression Series Part Four: Finding Shelter in an Uncertain World
In the final of this four-part series on the history and development of tech decompression protocols, GUE founder and president, Jarrod Jablonski weaves together various forays into decompression science, including Brian Hill’s pioneering pearl diver study, the NEDU’s work on deep stops, evidence of individual susceptibility, and probabilistic decompression models in an attempt to define the state of our understanding. It may give you pause to stop. Feel free to add your comments.
By Jarrod Jablonski
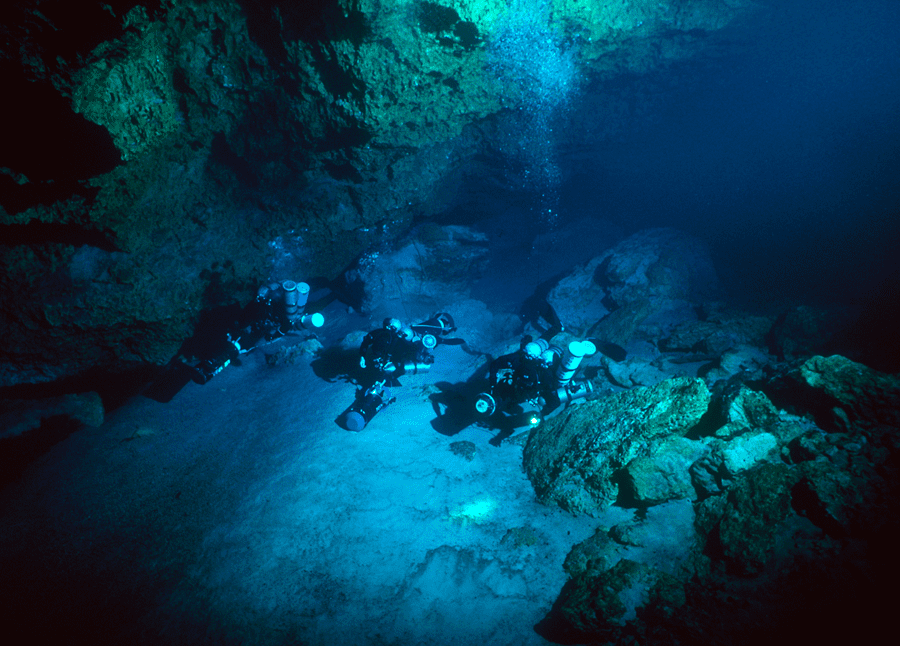
Header photo courtesy of the GUE archives
Did you miss: Part I, Part II, Part III
The human quest to explore below the water’s surface began some . Since that time, our species has pursued deeper and longer immersions, charting a course through hundreds of years of diving activity and associated research. Many of the advances in procedure, technique, and equipment are a direct result of the compelling and valuable data and experience documented during underwater explorations. As with many novel activities, this process of advancement required pushing physical and intellectual barriers.
During the 1980s and 90s, advances in technology supported an activity that became known as technical diving. This diving led to the development of ascent practices which were somewhat different from those of scientific, military, and commercial divers. A unique set of needs and limited relevant examples encouraged a great deal of experimentation among these early explorers, including adjustments to breathing gases and the distribution of decompression stops used during their ascent. Some technical divers began using a slower ascent from depth, in the hope this would control the formation of bubbles. These slow ascents became known as “deep stops” and were practiced in the hope they could reduce decompression stress and/or shorten decompression time.















In fact, the idea of bubble control was not new. During the 1960s, physiologist Brian Hills sought to characterize the profiles of pearl divers who had been operating since the late 1800s. These divers were interesting because they were ascending in two-thirds of the time required by Navy tables, a time that would cut even more decompression from most modern-day ascent schedules. Hills believed the reduced decompression times were the result of a unique ascent profile, including stops deeper than those called for by the Navy tables. Years later, technical diving explorers started adopting similar techniques while reporting reductions in total decompression time. It is difficult to qualify if this perceived success was actually occurring since the groups were relatively small, not carefully monitored, and simultaneously adjusting numerous other factors during their ascent. Even absent these complications, the generally low risk of decompression sickness can greatly complicate evaluations between different strategies.
The enthusiasm for deep stops likely reached its peak in the late 1990s and was dealt a serious blow by the previously discussed Navy Experimental Diving Unit (NEDU) study that was released in 2011. This study, and others, propose that deep stops are less efficient and may actually increase the risk of decompression sickness. The reader should refer to part three of this series for discussion and references. This series contends that opposition to deep stops is supported by prevailing research, but that a range of other variables need to be considered in order to effectively develop best practices. These aspects are particularly relevant to experienced divers, who report decompression sickness problems when eliminating slower ascents from depth.

It is not my intent to re-litigate the previous three sections of this article, but an interesting, and I believe, underappreciated aspect of Brian Hills’ pearl diver study provides a nice segue. What I find most interesting are the roughly 3,000 deaths and injuries of an unknown quantity that helped shape those unique ascent profiles. In other words, how was this conclusion affected by the elimination of those who are more susceptible to injury, and how much was due to a ? Hills concluded that the success of the profiles was “due to the much deeper initial decompression stops used” by the pearl divers. In a similar way, technical divers took note of the history, the encouragement from experts, and the perceived success by those in their community.
Given new and mounting evidence against deep stops, can we now definitively conclude that Hills, the pearl divers, and the tech divers were wrong? Are we sure the perceived success was imagined? If some success occurred, was it more about the generally low levels of risk in decompression sickness? Or could something else worth considering be at play? Asked another way, we might inquire how the conclusions reached by Hills and those technical divers are different from the way modern-day decompression tables have come into being.
The history of pearl diving and deep stops is very different from that of most decompression research in at least two substantial ways. The first difference has to do with methodologies, and the second with objectives. In terms of methodology, most decompression research is conducted using the scientific method: developing a testable hypothesis and, hopefully, crafting well-devised experiments in order to interrogate the hypothesis. Open publication of methods and results, internal and external debate, and reproducibility of results are among the many ways in which a hypothesis will be tested over time, narrowing the results toward either a more or less trusted conclusion. The history of deep stops, and possibly to a lesser extent, that of pearl divers, share few, if any, of the rigors commonly associated with the scientific method.
Individual Susceptibility
Looking to the history of decompression research, the objective of a particular study is implicit, if not explicit, in the development and testing of a hypothesis. With decompression profiles, we seek to balance the safety of the majority while not unduly affecting the whole. For example, we seek ascent profiles that keep a high percentage of individuals from being injured while not greatly extending the decompression time of the group as a whole. What would the results look like if we instead sought the most efficient decompression for a select minority of individuals?
Some researchers joke among themselves that they already know who will get bent among a group of test individuals. This is because research trials require a lot of volunteers among a relatively small population of willing participants, meaning that some of the same individuals are often involved in multiple experiments. This is not to say that a few individuals have skewed all research, but rather to say that a minority of subjects in all research projects can affect the outcome by being particularly susceptible to decompression stress.
This individual susceptibility is likely no surprise to anyone and is relatively well established among researchers, as is the variability in one individual from one day to the next. We see such variability in almost every conceivable area of our lives, affecting the way we respond to everything from drugs and alcohol to food and criticism. How could it be otherwise? We are all a kind of genetic experiment, refined through time with an endless series of personal and species-wide successes and failures. If we are variably sensitive to decompression stress, as seems almost certain, then in what myriad of ways might that be playing out?
It appears that some individuals bubble more and some less on the same profile. Might they also be more or less sensitive to whatever collection of bubbles are generated? Is it possible that we develop different collections of symptoms to various types of decompression stress? That we are individually more or less sensitive to similar symptoms? Some of these factors we believe to be true and some we might suspect to be true. Many others lurk in the background, and all impact our sense of what we might call decompression stress.

Given a world filled with individuals, we must do our best to bridge the divide. The good news is that we do this relatively well seeing that some differences are important but most are not usually extreme. The tail of the distribution represented by a small number of resistant individuals may well be quite small. This means that building profiles for resistant individuals might not have much impact and/or might be unreasonably dangerous. Either way, this individual variability is highly relevant and holds promise for the future. The next big advancement in health care will likely involve personalized medicine. Most of us may not live to see the usefulness of these developments in medicine, much less in decompression research, but the process is nonetheless hopeful. For example, research on heart rate variability might be one such development, allowing a theoretical computer to monitor your individual stress and adjust the ascent accordingly.
Managing individual susceptibility to a fluctuating range of variables is complicated, especially when many of these variables remain undiscovered, or at least poorly understood. Clearly, all is not lost, as we do a very good job managing the problem of decompression sickness. Depending upon our measure of success, we could say this problem is effectively solved. The fact that we are arguing about the nuances of decompression-stop arrangement and obsessing about relatively small adjustments to our total decompression time speaks to this success. We are likely refining along the margins beyond the point of diminishing returns. However, we should not fool ourselves into thinking that we have all the answers.
It’s The Data, Stupid
Another way to look at the science of decompression is to say it has mostly been a data-gathering exercise around which we fit slowly evolving boundary conditions. The boundary conditions are prescribed by algorithms and work quite well as long as we stay roughly within their range. It is quite possible we are not capturing any kind of truth about the way things work but rather refining our boundaries as we gather more data. It is true that we briefly foray into the field for some bubble-dynamics or that we strive to define the boundaries with process-markers like immune response, but none of these aspects has yet to produce a credible change in current practices.
By far the most useful part of decompression research has been the accumulation of data and the refinement of algorithms that capture these outcomes. Ideally, these algorithms would extend well beyond the data they describe, supporting “safe” diving profiles where sparse or even no data exists. Yet, evidence suggests that our models are especially bad in these outlier territories including very deep and/or very long dives. Most divers with meaningful experience in the 100+ meter range will admit they have little assurance of a clean ascent absent any symptoms of decompression sickness. These aspects further suggest that we are working in the proverbial dark, or at least just barely within the distant illumination of modern knowledge. This appears true at least with respect to specific determinations of cause (mistakes made) and effect (DCS incidence). Attempts to manage this uncertainty are in process among researchers spanning the globe.
Most experts are convinced that bubbles play a role in developing symptoms of decompression sickness, and most of these believe the effect is significant. In this regard, we have perhaps not come so far from Haldane or Buhlmann, who were both well aware of bubbles but lacked the tools to manage their development throughout a diver’s ascent. Likewise, the most recent deep stop studies do not propose that bubbles are irrelevant, only that deep stops appear inefficient and, in at least some cases, can increase risk. On the other side, we have evidence that slower ascents and/or deeper stops can reduce bubbling, but we remain unclear about the degree of importance the bubbling itself represents, especially over the long ascents conducted by technical divers.
Even a perfect model of bubbles might fail to predict or appreciably reduce decompression sickness, given the many complications in asserting the specific effect of bubbles in a given individual or within a particular injury. We are probably far from a perfect bubble model and perhaps even farther from determining how the wide array of variables might impact different individuals over time.
Perhaps we can find a way to manage our uncertainty while still progressing our understanding of the likelihood of a given outcome. For good reason, this process is reminiscent of mysteries coming to light in other fields. We seem to be discovering that more knowledge in a given area does not always result in a clearer understanding. Less than 50 years ago, most people were convinced we had “solved” the mystery of elementary particles, bundling the atom in nice packages of three constituents with simple-sounding names. Now the more we learn, the better we measure, the deeper we look, the more unsettling is the complexity.
Probabilistic Models and Uncertainty
Despite the confusing world around us, we have managed to achieve a high degree of success, and this continues despite our uncertainty. Management of this uncertainty can be mitigated by the use of and is currently common in other disciplines. This is an interesting and promising field, though it seems unlikely will greatly change our current decompression profiles. This assumption may be wrong but seems appropriate, partly because we already have very low levels of decompression sickness, and partly because we have many supporting dives validating current time/depth profiles.
Adjustments like deep stops temporarily promised to reduce decompression time, perhaps by as much as one-third, but failed to materialize when tested more rigorously. This seems likely to remain true, at least as long as we assert a primary objective in maintaining very low DCS risk for the overwhelming majority. There may be a variety of small improvements to be found, but our current approach seems broadly “correct,” at least within the bounds of most active diving profiles.
In some ways, we already manage uncertainty but do so indirectly by assigning a very low level of acceptable risk to the profiles that we test. This ultimately impacts the resulting decompression schedule. Using probabilistic models might allow us to permit a high level of risk, which could conceivably shorten decompression time. However, it remains to be seen if these models will be released in a way that allows users to accept high levels of risk. Even if such options become available, I wonder how many divers would use them in an aggressive way. Regardless of these factors, probabilistic models might allow a rational selection of risk, especially for those with the requisite understanding.
Current and foreseeable models may not be describing any sort of truth, but they do appear good at determining useful boundaries (time and depth limitations) around which a desired outcome (limited DCS risk) appears most likely. I do not mean to belittle that success in the least. We maintain a high degree of confidence we will not suffer decompression sickness on most dives, and that is no small achievement. Yet, it also brings us full circle and back to the idea that modern-day decompression tables are largely determined by those most susceptible to decompression sickness.
The NEDU study was stopped when it reached a threshold relating to DCS outcome. In this case, 10 of 198 dives resulted in DCS symptoms. Most were mild, late onset, Type I, but with two cases of rapidly progressing CNS manifestations. Two of the DCS cases were experienced by one individual. Ethical considerations require that a manned diving trial with DCS as an end point be designed to limit unnecessary injury to divers by maintaining a low level of DCS risk. This is a sensible and inevitable outcome of human trials.
I am not advocating for a change to this strategy, but I am curious how this process affects our understanding of DCS, since we know little about the reactions occurring in more than 90 percent of test subjects. Would these individuals begin experiencing low-level symptoms after longer exposures? How much longer? Would we suddenly start seeing dangerous Type 2 symptoms in a rapidly escalating percentage of individuals? This rapidly escalating risk seems likely based upon experience with provocative profiles, but the details remain poorly defined.

Maybe some individuals are more resistant to bubble formation while they or others are less sensitive to the bubbles that form. We can find many cases of prolific bubbling absent DCS symptoms. Meanwhile, DCS symptoms can be present with no detectable bubbles. This is to be expected, as symptoms are at least partly related to where bubbles are located. But these results might also hint at other differences in our response to bubbling. What if some divers form bubbles easily and/or experience high susceptibility to any formed bubbles? How would that knowledge affect any decompression recommendations? Is it conceivable that what works well for one diver or even the majority of divers is not optimal for all divers?
All of this ambiguity should lead a thinking person to question the certainty of their pronouncements. We might be inclined to reduce our deep gradient and ascend more quickly from depth, as the developing evidence indicates. But we should also respect the dive buddy that says they get bent when moving quicker in deep water. We can’t definitively say what works best, but we can say what seems to work well in the majority of cases for the majority of people. For most divers, these debates are largely academic, since the differences in profiles amount to minutes in one direction or another.
Technical divers are progressively more affected by changes in recommended ascent profiles in relation to the length of their dives. Yet, even tech dives of relatively modest lengths show impacts of less than 10 minutes and are usually not worth nearly as much anxiety as one can find in the community. Having said this, it is easy to appreciate the desire to maximize efficiency. I am merely trying to suggest one should not be in a big hurry to change what seemed successful in the past. Those wishing to balance experience with evolving science might begin to raise their deeper gradients in a progressive fashion over time while paying attention to how they and their dive buddies respond. Or a person that perceives success with their current approach might choose to hold tight and make few, if any changes. I am arguing that we should recognize both opinions have merit and that we should take each perspective into account when working within our team to establish a given ascent schedule.
The one definitive thing we can say about decompression is that it works well in the vast majority of cases, and when it doesn’t work, we probably will not know the exact reason. That reality is unlikely to change in the foreseeable future, although we certainly need to keep trying. A knowledgeable friend of mine once said that if we get bent, it is because we did not do enough decompression. Truer words have never been spoken.
Personal Note:
I am very curious to hear about your experiences and opinions regarding evolving decompression science. Are most of you convinced that deep stops bring no value? How many think they are dangerous? Do you think I make too much of individual susceptibility, or do you see that in your own experiences? I welcome all points of view, critical and otherwise. Let the games begin :-).

Jarrod is an avid explorer, researcher, author, and instructor who teaches and dives in oceans and caves around the world. Trained as a geologist, Jarrod is the founder and president of GUE and CEO of Halcyon and Extreme Exposure while remaining active in conservation, exploration, and filming projects worldwide. His explorations regularly place him in the most remote locations in the world, including numerous world record cave dives with total immersions near 30 hours. Jarrod is also an author with dozens of publications, including three books.























From Fear to Fieldwork: How Science Rewrites the Shark Story

By Divers, For Divers: The iQsub CCR Story

North, South, and Nowhere Warm

Spinal DCS: A Personal and Professional View

Technical Diving: Honoring the Man Behind the Name

Cave Biology: What Lives When Light Ends
