Featured
Decompression, Deep Stops and the Pursuit of Precision in a Complex World
In this first of a four-part series, Global Underwater Explorers’ (GUE) founder and president Jarrod Jablonski explores the historical development of GUE decompression protocols, with a focus on technical diving and the evolving trends in decompression research.
by Jarrod Jablonski
Introduction:
This four-part series will explore the historical development of Global Underwater Explorers’ (GUE) decompression protocols with a focus on technical diving and the evolving trends in decompression research. The series will include aspects important in recreational diving but with a greater focus on the variables affecting technical divers. Those with less technical experience will hopefully benefit from a substantial number of reference materials linked throughout the series. These support materials and the balanced perspectives I am striving to present are designed to encourage a broader grasp of this complex subject. I also wish to take a few chances with this series by presenting some controversial positions in the hope they will stimulate open discussion and deeper consideration on all sides.
In the interest of disclosure, I would like to foreground my belief that it is impossible to reach a definitive conclusion regarding the most efficient or the safest decompression procedures, though such determinations depend largely on how you define these terms. Indeed, it is a lack of certainty that motivates me to write this series since most of us will experience our entire diving careers with uncertain knowledge and while evaluating contradictory advice. It is my intent to provide a balanced overview while asserting that one should pursue a measured response to the dictates of pundits on all sides of the debate, myself included. Most importantly, I will explore the idea that many details may not be as significant as we typically imagine. For the sake of informed consideration, we will even explore the idea that both sides—in fact, all of us—are wrong and that we might know less about decompression sickness than it appears.
One last word on the structure of this series. My intent here is more about establishing a broad perspective and less about arguing a narrow view of this elaborate subject. To this end, I hope you will join the discussion by posting in our comments, or that some of these ideas might stimulate discussions in your various communities. Let’s get started.

















Part One: Contextualizing the problem of decompression.
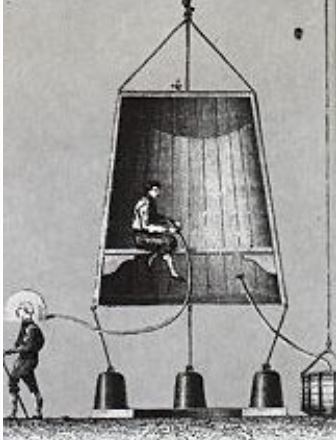
Humans have been exploring the underwater world for hundreds of years, driven by a seemingly insatiable curiosity to reach ever farther below the mysterious surface. The brevity of early breath-hold dives gave way to technology with advances in diving bells in the 16th and 17th century and led to the development of independent diving with the Fleuss rebreather unit around 100 years later. The Fluess device was a self-contained underwater breathing apparatus (scuba) and helped develop the future of untethered diving, although excursions would remain short and/or shallow for many years to come.

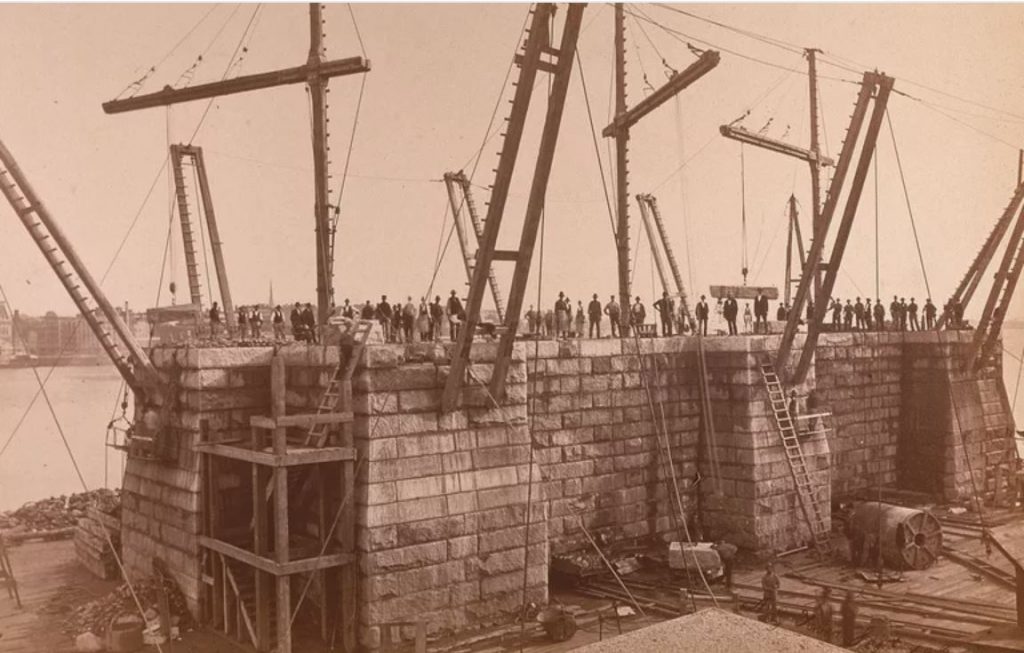
Developing technology that could support extended time while working underwater was a necessary part of the construction of bridges such as the Brooklyn Bridge during the 1870s. This was accomplished by constructing underwater rooms that were pressurized to keep them dry. Few people would think of these immersions as “diving,” but the extended time breathing gas at pressure highlighted a problem that would become known as decompression sickness, which was later included as one of two distinct pathophysiologies.
The desire to understand and ultimately prevent the occurrence of decompression-related injury spans the life and interest of many researchers, nations, and individuals. In order to better appreciate some historical context, we can refer to the early work of Robert Boyle (1627 – 1691) who identified pressure-related problems when he spotted bubbles in the eye of a decompressed snake. Those not familiar with Robert Boyle may be familiar with J.S. Haldane (1860 – 1936) who is credited with establishing the first set of decompression tables while under commission by the Royal Navy.
Meanwhile, individuals like Albert Buhlmann (1923 – 1994) helped develop the science of decompression during a rich university career, including work for military, commercial, and even recreational diving interests. Decompression enthusiasts are likely familiar with early work done by researchers like Brian Hills (1934 – 2006) who focused on incorporating the formation of bubbles into decompression algorithms. Certainly, these few people do not properly represent the science of decompression, and we could list dozens of other important individuals who heavily shaped the science. My intent here is only to highlight the span of more than 5,000 years during which humans have been reaching ever farther below the watery surface. This history also includes roughly 200 years of research by a wide range of individuals, organizations, and governments seeking to understand the complications of breathing gas under increased pressure.
The development of decompression practices proved successful even in their first use with caisson work, notably reducing the problems associated with breathing gas while under pressure. This progress extended into diving activity, and included the first tables produced by Haldane in 1908 for the British Admiralty. His tables remained in use by the Royal Navy until 1955. These developments supported longer and more aggressive diving activity, inaugurating a new age of discoveries and their associated challenges.
Advancement tends to remove some or even many risks but also creates the possibility for new problems. These might develop from the ability to push boundaries farther or because more people can become involved in a given activity. We tend to build upon early success, refining safety protocols and treating a progressively smaller subset of incidents. Over time, the strategies to reduce injury become more refined and, to some extent, more individualized.
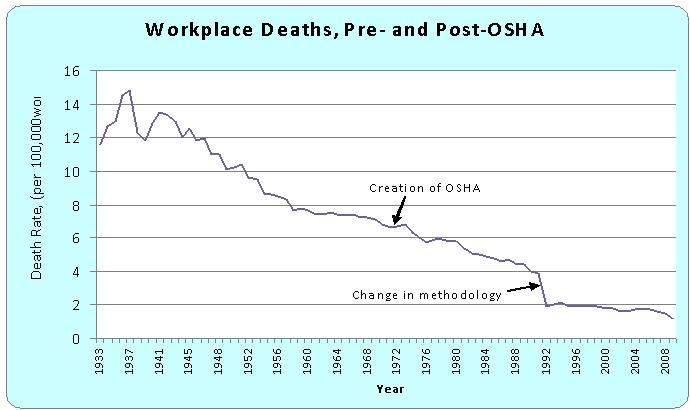
For example, early cities were very dangerous places before fire protection, building standards, health codes, and similar protections. These practices became more refined, focusing on workers, home dwellers, children, and others. Most advanced societies are now quite safe, and additional levels of refinement continue to tease individual safety concerns while striving for the elimination of accidents—requiring notably more effort and expense to remove progressively smaller amounts of risk. It is hard to clearly identify our place on this curve when it comes to decompression sickness, but we appear fairly well into the diminishing returns part of the process.
Exploring high-pressure environments began when elaborate mining, tunneling, and bridge-building projects resulted in problems of unknown origin. In subsequent years, we identified an arguably well-defined illness with a relatively clear causality. Many details remain vague, but our ability to characterize the problem supported the development of decompression strategies that significantly reduced injuries associated with breathing gas under pressure. These developments resulted in algorithms that predicted safe exposures and were codified into decompression tables and used for progressively deeper diving excursions.
Today, decompression-related problems are extremely uncommon, especially within the recreational diving community. We now find ourselves mostly managing problems within a small subset of incidents. We strive for clarity among these low-probability injuries, seeking to improve or at least maintain safe guidelines while expanding our understanding. We typically acknowledge some influence from pre-existing conditions that, for whatever collection of reasons, might make a person more susceptible to injury. We also strive to discourage diving activity that violates defined ascent speed or time limits while trying to establish a solid understanding of the constellation of problems we call decompression sickness.
Meanwhile, the safety of decompression among those who use algorithms within uncharted territory remains less certain. Individuals who dive very deep and/or over very long times may be outside the range where safe dives can be predicted. For example, a decompression algorithm developed for dives up to 30m/100 ft for immersions as long as one hour may or may not extrapolate for dives of longer duration and depth. It requires a great many dives in order to verify that a particular exposure will result in low risk for most people. Given the high cost, added complexity, and safety risk, these important data points are particularly limited with dives that are very deep and/or long. This is something we return to in a later discussion.
For the moment, we are mostly focused on dives with good supporting data and where notable improvement appears unlikely. Much of the sometimes raucous debate over decompression “correctness” involves teasing arguably minor benefits from already very low levels of risk. Can we change this reality? Can we find something that brings substantial improvement, perhaps allowing much longer dives with even shorter decompressions?
In thinking about the “problem” of decompression, we understand that scuba diving increases the pressure around us, also known as increased ambient pressure. We are now breathing gas that is at a higher pressure than normally exists in our body. The molecules we are breathing become dissolved in our blood, where they are transferred during normal circulation and accumulate in the tissues of our body. This occurs until the tissues are “full” or, more precisely, until they are saturated at the new inspired gas pressure. Reductions in the surrounding pressure reverse the gradient and encourage the molecules to leave the tissues through the blood.
Algorithms that strive to characterize this process are known as dissolved gas models. The transfer of dissolved gas from the tissues often results in the formation of bubbles in a way that is similar to releasing pressure from a carbonated beverage. Dissolved gas models do not ignore the risk of bubbles but also do not attempt to directly control their development. Attempts to directly limit the formation and development of bubbles are known as bubble models.
We imagine that both dissolved gas and bubbles are relevant and also that other individual factors play some role. The problems in finding the best strategy are numerous, but most will be managed in a later discussion. For now, I wish to highlight that tracking of dissolved gas has been our primary strategy, consuming all but a relative handful of the many decompression experiments through the history of decompression research.
Modeling bubbles is inevitably more theoretical and based upon mathematically derived predictions about bubble behavior, sometimes supported by lab experiments that measure the likelihood of bubble formation under certain conditions. Models can also be crafted as “dual-phase,” meaning they anticipate bubble development but also track dissolved gas, striving to ensure that both are within safe parameters. In all cases, we tend to develop more confidence in models that are tested empirically, though they may also be compared to a database of outcomes, supporting evaluation and calibration of the model particulars. The most modern approach is trending toward probabilistic models, and we will explore these in future treatment.
The presence of bubbles during decompression is well known, and to some extent is measurable by Doppler testing, which can detect bubbles in the venous part of the circulatory system. The venous system receives blood from tissues that are eliminating gas absorbed while diving, so the presence of at least some bubbles are expected. Unfortunately, there are many complications to the use of Doppler as a means to gauge decompression efficiency. Measures of venous bubbles may be useful for predicting decompression stress in populations of divers, but it fails to be a reliable measure of symptoms in an individual diver.
Despite the complications, most researchers agree that bubbles (though not necessarily those detectable in the venous blood) are a critical part of the causal chain. The consensus seems to be that these bubbles either directly cause decompression sickness and/or contribute to its severity. Even if we assume bubbles cause all decompression-related symptoms, predicting their effects might be overly complicated. Albert Buhlmann, a great contributor to dissolved gas models, knew about and acknowledged the relevance of bubbles. He nonetheless focused upon refining dissolved gas strategies as a way to minimize risk of decompression sickness. We don’t yet know if this is the best strategy, but it has been quite successful at allowing a very low level of risk during most dives.
Tracking other markers that might affect symptoms of decompression sickness is conceivable and is part of a body of research that seeks to better understand the full scope of decompression problems. For example, researchers are exploring immune-response factors, including genetic influences that might be involved in the body’s reaction to decompression. We might also learn more about heart rate variability (HRV), which has become popular as a way to measure physiological stress in the world of sport and exercise, and its potential involvement in DCS. These or other techniques could conceivably be used to establish upper limits on the stress accumulation that occurs during decompression, presumably avoiding some upper threshold before symptoms become problematic.
We might also find ways to reduce decompression time by eliminating or changing the gas at the source of the problem. For example, we might eventually manage to use a liquid carrier for the oxygen that sustains our lives. By eliminating or greatly reducing use of gases like nitrogen or helium, we should be able to notably change the relevance of bubbling during changes in pressure. Or, we might develop ways to prevent or greatly reduce the risk of bubble formation by using drugs or other prophylactics that could physically alter the circumstances under which bubbles form. These ideas and many others have been explored and may hold promise, but nothing that greatly departs from current practice appears likely in the foreseeable future.
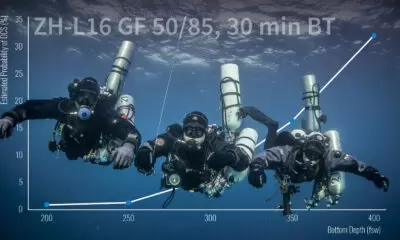
Despite reasonable uncertainty about many details in decompression sickness, including the exact incident rate of DCS, which is unknown, divers following conventional decompression tables and diving within well-established limits have a very low risk of injury with rates of 0.01-0.1% per dive or about 1-10 incidents per 10,000 dives (the higher end reflecting rates for commercial dives, the lower end reflecting technical, scientific, and recreational dives). The risk is greater for certain types of very aggressive dives, but we will explore that aspect in a later discussion. Regardless of the actual risk, few divers would knowingly choose a less efficient ascent profile if a better option was available.
The pursuit of decompression efficiency is particularly relevant for the group of divers known as technical divers. For these divers, arguably small differences can involve additional hours decompressing in the water. These divers have been particularly interested in the problem of bubbles that might develop during long ascents in deep water. Many tech divers followed early research that concluded slower ascents from depth could greatly reduce decompression time. For some years, the convention of using “deep stops” to slow a diver’s ascent seemed to be the best way forward. Yet, new research argues they are actually part of the problem. Whether or not you feel sure about the value of deep stops, I hope you will join us for some engaging online discussions and especially for future sections as we dig deeper into areas that do not commonly appear in discussions orbiting decompression or deep stops. I look forward to reading your thoughts in the comments section and hope you will join part two of our series: “Tech Divers, Deep Stops, and the Coming Apocalypse”.
Part II: “Tech Divers, Deep Stops, and the Coming Apocalypse”
Part III: Bubble-wise, pound-foolish. Are deep stops dangerous?
Part IIII: Finding Shelter in an Uncertain World

Jarrod is an avid explorer, researcher, author, and instructor who teaches and dives in oceans and caves around the world. Trained as a geologist, Jarrod is the founder and president of GUE and CEO of Halcyon and Extreme Exposure while remaining active in conservation, exploration, and filming projects worldwide. His explorations regularly place him in the most remote locations in the world, including numerous world record cave dives with total immersions near 30 hours. Jarrod is also an author with dozens of publications, including three books.



























Dial In Your DCS Risk with the Thalmann Algorithm

Deep Tunnel Workers Go Trimix

La Grande Dérive

California Dreamin’

British Invasion—Thailand Karst Edition 2024

Harnessing the Power of ‘Educated’ AI to Improve Diving Safety
