

Latest Features
Pioneering Portable Chamber Technology
Has the time come for portable chamber technology? I thought it had in JAN 1993 when we made the SOS Hyperlite chamber the cover story of aquaCORPS Journal #5 BENT. Fast forward 32 years, and the Hyperlite is now near ubiquitous among mobile military divers, but noticeably absent among the tech community. Can a business model be found? Dive med tech Jen Howard explains the history, development and uses of SOS’s portable chamber, and reviews several cases.
By Jen Howard. Images courtesy of SOS GROUP unless noted.Lead image: SOS founder John Selby assisting with a diver evacuation.
The SOS Group – inventors of Hyperbaric Stretcher – the go to system for hyperbaric evacuation for the US Military – is celebrating 35 years in business.

Founded by John Selby in 1987, the SOS Group revolutionized the hyperbaric scene with the development of the Hyperlite 1, the first flexible, lightweight chamber capable of transporting a diver suffering from decompression sickness under pressure by sea, land, or in a helicopter up to 5,100 m/17,000 ft. The technology was even featured as the cover story of aquaCORPS Journal #5BENT.
Decompression Sickness (DCS) is caused by the formation of nitrogen bubbles in the body’s tissues and blood; these bubbles cause blockages that prevent normal body functions. Bubbles usually form during pressure drops in a person’s surrounding environment; bubble formation is particularly prevalent underwater, where significant pressure changes occur as divers ascend to shallow water.

The concept of recompression for treating DCS was first discovered during the excavation of the Hudson River tunnel in 1854. Construction workers, after working in pressurised environments, would suffer from symptoms of what they called “‘the bends”—a reference to the way DCS victims bent over in pain. This posture resembled a Grecian Bend, a fashionable female posture during the 19th century. The construction company realized that, when an individual was put back under pressure, symptoms would subside. Although they didn’t know it at the time, repressurization dissolved the nitrogen bubbles in the body back into solution.
By the early 1900s, hyperbaric chambers had become essential equipment for all compressed air operations. Made from steel, early designs were developed to feature an entry compartment attached to a main compartment to allow a patient and their carer (now referred to as a tender) to be transferred in and out for treatment.
Recognizing the benefits from the construction industry, manufacturers began introducing recompression chambers into the naval and commercial diving scene. Logistical challenges associated with offshore activities led to further technological developments, with smaller transportable aluminum pressure vessels offering a lighter alternative to traditional, fixed, multi-occupant chambers (known as multi-place chambers).
Growing demand for underwater works in confined spaces and remote locations led to the introduction of the single occupancy or “mono-place” chamber. Made from traditional metallic pressure vessel materials to form a pressure-retaining hard shell, mono-place chambers reached the same pressures as their multi-place predecessors. Equipped with a lock-on device, the mono-place portable systems were designed to be coupled to multi-place chambers (usually located in fixed, land based facilities) via a compatible flange connection.
After locking together, the chambers would equalize to allow a patient transfer. Unfortunately, the single recompression chambers were still inhibited by several limitations. They were too heavy, difficult to mobilize and store, and, with a small, six-inch window, were extremely dark and claustrophobic. The unwelcoming capsule did, however, present a useful deterrent to placate an over-adventurous diver before entering the water. Additional problems—due to inconsistencies in flange designs, shapes, and sizes—made the connecting of chambers very challenging or completely unfeasible (a problem that still exists today).

The rapid expansion of Navy diving activities during the two World Wars saw significant advancements of subsea equipment, including submarine operations and tactical diving. Recompression chambers became common onboard larger vessels for regular diving operations, but the distance between operational activities and the nearest chamber remained an occupational risk. In some cases, even aeromedical evacuation was infeasible due to exposure at altitude exacerbating the symptoms of decompression sickness.
For hyperbaric treatment to be most effective, it needed to be as close to the point of injury as possible; and, if full hyperbaric capabilities on-site were not feasible, a method for safe aeromedical evacuation was the next best option, allowing the patient to remain stable while improving symptoms before comprehensive care was available.

Developing the Hyperbaric Stretcher
While running a diving equipment wholesaler with his wife Jane in London in the late 1980s, the challenges of hyperbaric chamber logistics led inventor and mechanical engineer John Selby to consider the application of high-strength textiles as a material for a lightweight pressure vessel for emergency evacuation. At the time, London Underwater Centre (LUC) was importing various equipment—mainly from Italy—including Coltri Compressors and Strumenti Ottici Subacquei (SOS (Italy)), translated as Optical Diving Instruments. Some may remember SOS (Italy), based in Torino, as the manufacturers of the first automated dive decompression meter. InDepth published an article about this in April 2022.
When SOS (Italy) closed for business, LUC acquired the rights to the name SOS and a prototype aluminum-bodied, portable hyperbaric chamber. This provided John with the basis for the concept of a portable chamber with a filament-wound silicon rubber pressure vessel, and he branded it the Hyperlite Hyperbaric Stretcher.
The company rebranded as SOS Ltd in 1989 and first received funding from the UK Defence Research Agency for building the first prototype Hyperlite. The chamber successfully completed a test program and entered service. The system received US Food and Drug Administration 510(k) Pre-Market Notification, allowing it to be supplied on the US market. Approval of a safety case under the American Society of Mechanical Engineers Safety Committee for Pressure Vessels for Human Occupancy (ASME-PVHO) followed, as well as completion of a US Navy-led Foreign Comparative Test Program, describing it as the Emergency Evacuation Hyperbaric Stretcher (EEHS).
The Hyperlite 1 featured a collapsible design; it could be folded and stored in two cases. With a diameter of just 58 cm/23 in and 2.4 m/8 ft long when assembled, the fabric chamber weighed in at 68 kg/150 lb and could be carried by four or six people to mobilize the system for evacuation. The diameter was limited so that the chamber could be passed through a traditional entry door of a fixed chamber, no longer requiring a connecting flange.
Assembled and pressurised in less than 15 minutes, the chamber is capable of operating pressures of up to 3.3 ATA, enough to meet the minimum pressure requirement of 2.8 ATA required to provide a US Navy Diving Treatment Table Six for decompression sickness. Such a pressure is necessary to dissolve nitrogen back into solution before inhaled oxygen displaces nitrogen, which is expelled naturally during exhalation.
Lightweight, robust, and suitable for deployment, the Hyperlite 1 was confirmed to be suitable to carry out a full US Navy Treatment Table 6 up to 5,273 m/17,300 ft in an unpressurised air cabin. Passing all the FCT tests, SOS Group’s flagship product was awarded US Navy Diving & Manned Systems and US Air Force approval for flight after undergoing aeromedical and human factors evaluations.

The Hyperlite in Action
Reported evidence of the Hyperlite 1 in action has showcased its efficacy and efficiency in mitigating fatal risks which could have been sustained in its absence. One being in August 2005, when a diving research expedition set out to two dive sites: an unidentified two-masted schooner and the wooden passenger steamer Pewabic, both resting in about 50 m/165 ft of water. Following diving protocols, a Hyperlite 1 was carried aboard the 12 m/39 ft diving vessel to meet the 30-minute dive protocol deadline. During one of the dives, a technical deep diver suffered severe DCS and required emergency, on-site hyperbaric oxygen therapy. The patient made a full recovery and was not compromized by any further limitations.
Another well-documented scenario occurred when world-recognized adventure diver Paul Rose was filming a documentary off the remote Pacific coral island of Niue and encountered a DCS incident which could have ended his diving career. He had been diving to only around 25 m/82 ft from an RIB and, while continuing to ascend after a safety stop at around 10 m/30 ft, was instantly paralysed on his right side and in part of his chest. Paul was immediately transferred back to the mothership and placed on surface oxygen. The team secured him inside the Hyperlite 1 and worked through the treatment protocol. With an oxygen mask on his face, he was pressurized to 20 m/60 ft and soon regained control of his limbs. Other symptoms subsided, as well. He made a full recovery and is back diving today.

Over the last few decades, SOS Group has gone on to provide portable hyperbaric solutions throughout the world, supplying military, law enforcement, and emergency services while also looking at ways to combat DCS incidents occurring with recreational diving—specifically those aboard larger yachts which have the resources and accountability to support their crew and clients when diving in remote locations.
Innovation and curiosity at the company’s heart, SOS Group is now led by Paul Selby, the founder’s son, who has overseen the development of an expanded portfolio of three products, including the improved Hyperlite 1 portable chamber—which now features an upgraded lightweight tube integrating braided Vectran® technology, improving durability and reducing the overall weight. In 2019, SOS released their first ASME PVHO-1 Case 18 Compliant, lightweight, single-lock hyperbaric chamber designed for multiple occupants, branded as the Hyperlite SL3. Suitable for hands-on medical attention, the chamber can be designed to reach operating pressures of up to 6 ATA, which is still occasionally used for treating severe DCS.

Alongside the SL3, a Double Lock version was developed specifically for the US Navy: the Multi Occupant Flexible Recompression Chamber System (MOFRC(S)). “The system retains the company mission of providing foldable lightweight systems that are quick to assemble and simple to operate” explained Selby. “The US Navy MOFRC(S) (or the Hyperlite DL5 models) offer a ‘pound-for-pound’ replacement to traditional Double Lock ‘Portable Recompression Chambers,’ the main difference being the number of pounds in weight that the end user is required to carry.”
A Double Lock chamber provides the advantage of an outside medic being able to enter and exit the chamber throughout a treatment. Both the SL3 and the Double Lock versions can carry up to 3 personnel in the main compartment, with the Double Lock being able to carry an additional person in the second compartment.
Portable Chambers vs. IWR
Despite the ongoing hyperbaric developments, success stories, and growing clinical evidence demonstrating hyperbaric oxygen treatment as the definitive treatment for DCS, there has been much discussion about recompression treatment via returning divers to depth in the water, known as in-water recompression (IWR). The main concept behind IWR is that it provides a rapid alternative to treat DCS in the absence of a recompression chamber.

According to Selby, “IWR involves reentering the water to return to depth where the diver breathes oxygen, if available. The practice adds complexity to an already complex situation, increasing the risk of central nervous system oxygen toxicity, which evidence has shown to be more prevalent when conducting strenuous activity,“ he said. “There is also a need for dedicated equipment and specialist training by skilled operators to support a diver in the water for hours of treatment and it carries an increased risk of hypothermia, which leads to further dehydration and affecting the vascular system which can worsen the symptoms of DCS. There is also an increased risk of drowning if the diver condition deteriorates; and [requires consideration of] the added variables of changing weather conditions.”
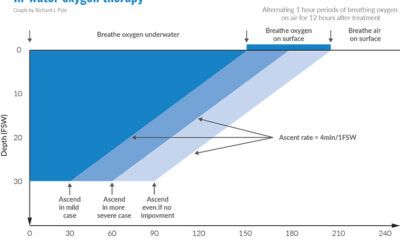
Our research found that of the few guidelines that cover the subject, some suggest carrying out IWR at shallower depths no more than 9 msw/29 fsw, for shorter durations (1-3 hours): conditions which are less likely to result in complete resolution of symptoms.
A paper published by Drs David Doolette and Simon Mitchell in 2018 (see below), suggested that the risk of IWR is not justified for treatment of mild symptoms which could potentially resolve without medical treatment or for divers that are in such critical states that they would not be safe in the water. However, for those sufficiently trained and with the correct equipment, it could potentially be justified in situations which are threatening to life or limb, when the option of timely recompression via hyperbaric chambers is unavailable, and or more than two hours away. It is in these circumstances that having a portable, lightweight chamber onboard could prevent having to make these decisions.













To most, having a Hyperlite 1 will appear as a luxury: a piece of equipment only required for military operations or commercial projects or perhaps only attainable by the ultra-wealthy onboard large yachts. “From a historical perspective, this is accurate,” Selby said. “This is where SOS Group receives the majority of our business. However, when the medical implications of delaying treatment are considered, alongside the ability to access locations further afield, both recreational and commercial sectors are beginning to think twice before relying on the nearest hyperbaric facility for treatment of DCS.”
As was explained in “Hyperbaric Chambers Are Turning Away Divers. Will There Be One Nearby When You Need It?,” in the September 2023 issue of InDEPTH, there has been a sharp decrease in the number of hyperbaric treatment centers willing to treat divers for DCS, even when it is life-threatening. According to DAN, in the US alone there are an estimated 1,500 hyperbaric medicine facilities, yet only 67 are currently treating dive incidents. This is understandable; between profitability concerns, the greater legal liability involved with treating acute patients, and the increased need for appropriate training and staffing for dive related injuries, medical facilities don’t prioritize dive medicine for a number of reasons.

A Critical Safety Issue
For the sport diving community, this is a critical safety issue. There are currently around three million recreational and technical divers in the US, with more visiting from overseas to visit unique sites around the coastlines and even further afield. As Selby explained, “In the event they suffer a dive-related injury, most will have assumed that there are hyperbaric chambers within required proximity to treat them. However, this is not the case, and they could endure huge delays in treatment and costly transportation to distant available facilities with unknown operators, chamber conditions, and opening hours.”
“For the commercial industries supporting diving tourism, particularly the liveaboards, there is a duty of care to the crew and the clients that organizations have a plan in place for hyperbaric treatment. It is not enough to say that, because there is no regulation to state that they need one, that they don’t. I would recommend that you ask about the emergency care plan and understand the risk before signing up for the package,” Selby said.
In 2020, The Undersea and Hyperbaric Medical Society, in partnership with the American College of Surgeons, the American College of Emergency Physicians, the Divers Alert Network, the Academy of Underwater Arts and Sciences, and others, wrote a letter to the President, select cabinet members, and elected representatives both in Congress and at the state level to bring this to their attention. The letter highlighted that, on average each year, there are 400 serious cases of DCS, around 1,000 reported cases of arterial gas embolism (AGE) as a result of medical or surgical procedures, and 13,000 cases of life-threatening soft tissue infections.
In May of 2020, a retired Marine Corps aviator made a dive to 21m/70 ft for 20 minutes off the coast of Pensacola, Florida. He was battling a large speared fish near the end of his dive. After surfacing, he experienced serious neurological symptoms that were indicative of a diving-related injury, but none of the five hyperbaric treatment facilities in Pensacola currently provide the emergency HBO2 therapy that he badly needed.
Knowing that no hyperbaric treatment facilities in the city or in the rest of Northwest Florida would treat the injured diver, his dive buddy, a retired Navy flight surgeon, arranged for him to be transported to the hyperbaric facility at Springhill Medical Center, in Mobile, Alabama, the closest treatment facility that offers emergency HBO2 therapy, where he was treated successfully
Steven Wells, on the other hand, was not so fortunate. During a dive, he proceeded to embark upon a rapid ascent causing DCS. Despite attempts to seek treatment, he was turned away from the nearest hyperbaric chamber due to lack of staff. Again, after multiple rejections from the nearby facilities, he elapsed the time frame required for urgent treatment, which cost him his life.
It is a sad and timely reminder of the changing environment for the sport diving community and, while typical portable chamber system costs start at $90,000 (not insignificant), it is a small price to pay when considered against the consequences. If nothing else, it is more important than ever to do the research, prepare for the worst, and hope for the best: a spectacular dive without incident.
Ed note: Perhaps the technical diving community can find a way to fund these chambers for remote expeditions, for example through leasing or a rental program. Wet Mules? Nixie? Are you listening? SOS Ltd is already working with a group conducting an expedition to Chuuk next year.
DIVE DEEPER
Website: THE SOS GROUP
aquaCORPS: Portable Chamber Technology by John Selby. Here is the original SOS article as it appeared in aquaCORPS #5 BENT (JAN 1993)
Diving and Hyperbaric medicine: In-water Recompression, Doolette DJ and Mitchell SJ (2018)
InDEPTH: A New Look at In-Water Recompression (IWR) by Reilly Fogarty
InDEPTH: Hyperbaric Chambers Are Turning Away Divers. Will There Be One Nearby When You Need It? by Ashley Stewart

aquaCORPS #5 BENT was published in JAN93 in conjunction with the first technical diving conference, tek.93, held just before the annual DEMA show in Orlando, Florida. The issue focused on decompression illness (DCI) and presented the latest thinking on the theory, classification, treatment, and human factors associated with DCI. Sponsored by DAN Europe.

Starting out her career as an international competitive swimmer, Jen Howard has worked as a freelance journalist for several publications including; Sky Sports, Dennis Publishing and Newsquest newspapers. A qualified trauma and first response nurse, Jen has been an Advanced Open Water diver since her childhood, diving all over the world, including wrecks in the Caribbean, the Great barrier reef in Australia, Fiji, Spain and the UK. Recently, she has taken an interest in the world of hyperbaric systems and after qualifying as a Dive Medic Technician, has worked as a medical chamber operator on a number of tunnelling projects in the UK.






















From Fear to Fieldwork: How Science Rewrites the Shark Story

“Deeper” with Dr. Richard Harris: A Movie Review

By Divers, For Divers: The iQsub CCR Story

Beneath the Jungle: The Connection That Changes Everything

North, South, and Nowhere Warm

Spinal DCS: A Personal and Professional View
