Community
No Fault DCI? The Story of My Wife’s PFO
What does it mean if you keep getting bent, even when you follow all the rules? Avid tech instructor James Fraser recounts his wife’s (Deana) and his own journey of discovery that led them to realize she had a PFO. Does any of this sound familiar? Read on!

by James Fraser. All photos courtesy of James Fraser
When you follow all the rules and still get decompression illness, what’s up?
The person I hold most dear in this life has now had three incidents of decompression illness (DCI) over a two-year period. The latest episode required recompression, so we began investigating her frequent illness to determine if there was a possible solution. Deana is a very conservative diver, diving within her training, computer limits, and dive planning tools such as Deco Planner. On all of the dives where she had DCI, her training, tools, and dive profiles say she should not have gotten bent. But she got bent just the same.

DCI is a risk for any diver, even when following the rules. However, we have to remember that DCI is a potential sports injury, no different than a football player risking a concussion. Despite this fact, DCI seems stigmatized, and people feel ashamed to admit it happened to them. So Deana and I decided to share her experiences with DCI, to help others realize, Sh*t, I mean, DCI happens! Experiences with DCI should be shared, so that the diving community can continue to learn, grow, and be safer divers.
Some background
Deana Fraser has been a registered nurse (RN) for over 25 years, and received her BSN in 2002. Throughout her career, she has specialized in ER, ICU, and OR nursing. Currently, she manages the Overlake Operating Roomin Bellevue, Wash. When Deana is not managing the OR, she is usually diving in the extreme conditions of the Pacific Northwest (PNW), where all dives are cold (46-55℉/8-13°C), dark, and wonderful. Deana has been a recreational diver since 2004, and loves diving in Seattle and the surrounding areas as often as three days a week. It is her number one passion.
She just completed her Global Underwater Explorers (GUE) Technical 1 course (normoxic trimix) in September 2019, and as of this article she has completed over 500 dives, 150 during 2019 alone. Deana always looks forward to expanding her skills and experience in the recreational and technical diving arena.















Deana is also a breast cancer survivor; she was diagnosed with Stage Two breast cancer in May 2016, and underwent a lumpectomy and six weeks of radiation treatment, until July 2016. She is in full recovery, but continues to take Tamoxifen (20mg) daily. This information is not intended to draw any type of correlation of breast cancer and DCI, but to give all details about Deana’s fitness and health in respect to her history with DCI.
Deana is one of those people that lets nothing hold her back. She was not able to dive for a few months after her radiation treatment, so she turned to her second love: hiking. She proceeded to hike over 200 miles (dragging her husband with her) over the next six months while she was recovering. Deana has been cancer free for over three years now and is back to her first love of diving. When she returned to diving, she pursued her dream of technical diving and signed up for GUE Fundamentals in 2017. She has been unstoppable since then and again has dragged her husband along for the ride.
After cancer treatment, Deana spent a lot of time building up her strength and dexterity in order to pack double 100s over the rocky beaches of the PNW. She trained relentlessly to reach the goal of being a GUE Tech 1 Diver, a mission that she accomplished. In addition to her regular dives, Deana leads a weekly Skills Refinery Dive, offering opportunities for other local divers to hone their techniques and commit to excellence. Many are working on their GUE Tech skills to prepare for Tech 1. Deana is not done with her education and has dreams of completing GUE’s Tech 2 course in the future. Now that you know the type of person Deana is, let’s talk about the reason she and I have written this article.
Look, James. I Got Stung by Something!

Deana and I went on a 16-day trip to the Maldives in April 2018. We spent the first week at Olhuveli Beach Resort resting, flipping our internal clocks, and doing a few recreational shore and boat charter dives. The second week, we joined up with our local Seattle dive group on Blue Force One, a fantastic live-aboard charter, for seven days of additional recreational diving; no dives on this trip were below 100 ft/30 m. On day three of diving on Blue Force, after her second dive, Deana talked to me about being stung on her abdomen. She presented with redness, point tenderness, and stinging in an area about the size of a silver dollar. She was wearing a full length 3mm wet so it definitely was not something she would have brushed against during the dive. She took a Benadryl, feeling that something stung her, got some sleep, and by the next morning it had cleared up. Deana continued diving for the rest of the trip and had no further symptoms. We now suspect that she had a minor case of skin bends, based on the other two episodes she has had since.
Deana and I also dived in Loreto, Mexico, six months after the Maldives, in October 2018, and performed ten dives over four days with a max depth of 80 ft/24 m; Deana showed no symptoms of DCI.
Could I Have Skin Bends?
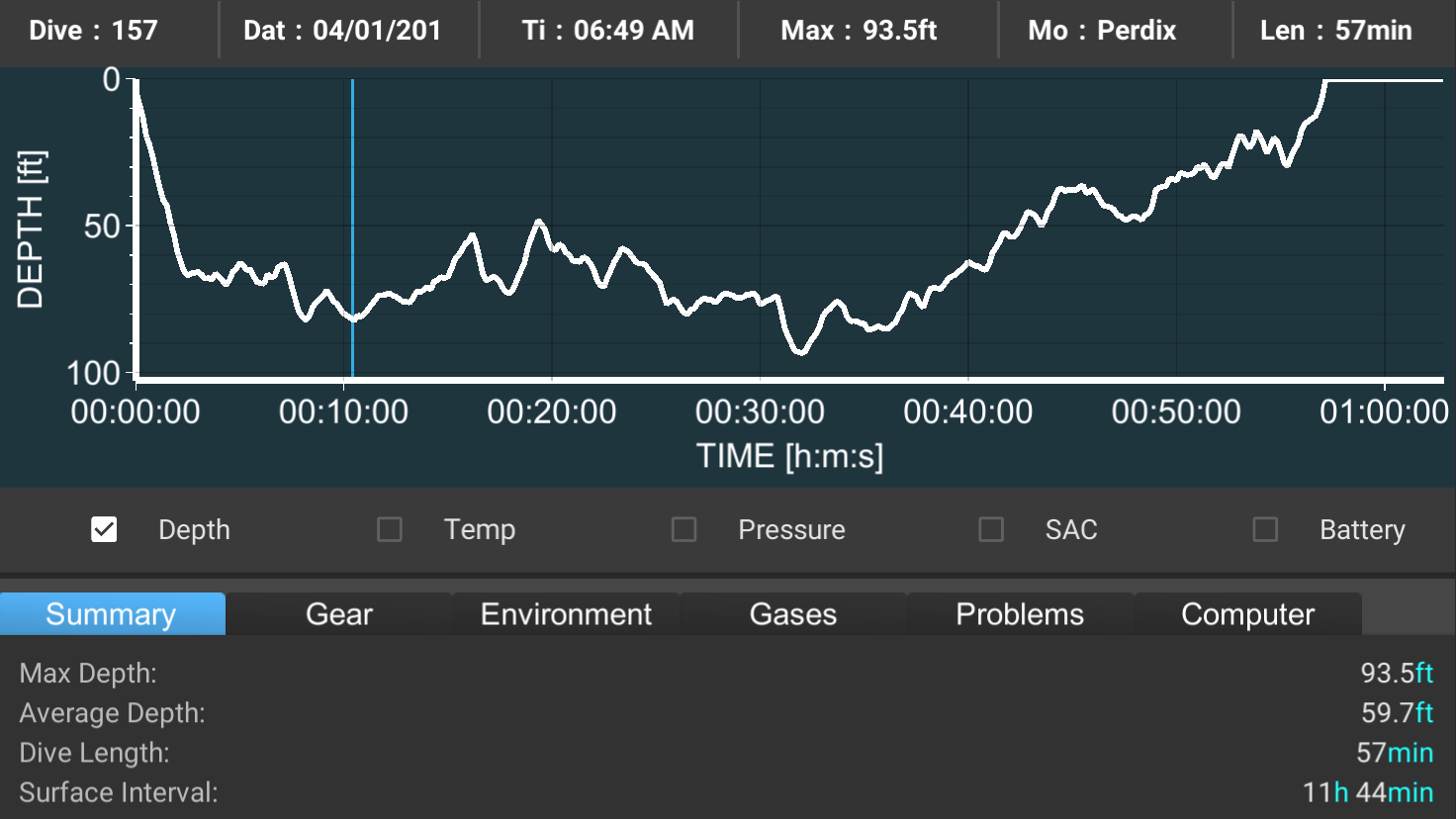
In April this year, 2019, Deana and I were in Hurghada, Egypt, on a live-aboard dive trip with Red Sea Explorers aboard MV Nouran. Deana had completed eight recreational nitrox dives over three days, the deepest dive being 98 ft/30 m, when she showed signs of skin bends. Below are the dive profiles of the two dives the day she presented with skin bends. She again had symptoms of stinging and itching on her thighs and abdomen and point tenderness. The area was larger than the first experience she had in the Maldives.

Deana again wondered if it was some kind of sting or allergic reaction and asked me and some of the more experienced divers for our opinions. A couple of the more senior technical divers on board agreed: Her symptoms looked and presented like skin bends. Deana went on 100% oxygen (O2) for a few hours, and the symptoms went away. She took the next day off and then continued to dive recreationally with more conservatism for the remainder of the trip. One other person on the trip who was doing Tech 1 level dives also showed signs of skin bends; they were treated with O2 and continued to dive for the rest of the trip with no further issues.
After this episode we thought about the Maldives: Since it presented the same way and resolved itself with some time and O2, we now assumed that was also an incident of minor skin bends.
Skin Bends Again, But Nothing a Bit of O2 Can’t Fix
Deana and I were attending Tek week at Buddy Dive in Bonaire. We were both looking forward to a week of Tech 1 dives (Max depth 170 ft/50 m, max deco: 30 min), as this was Deana’s first trip since passing her course. We had done three dives total over days one and two at recreational depths on nitrox 32 (32% oxygen, 68% nitrogen) with no required deco.
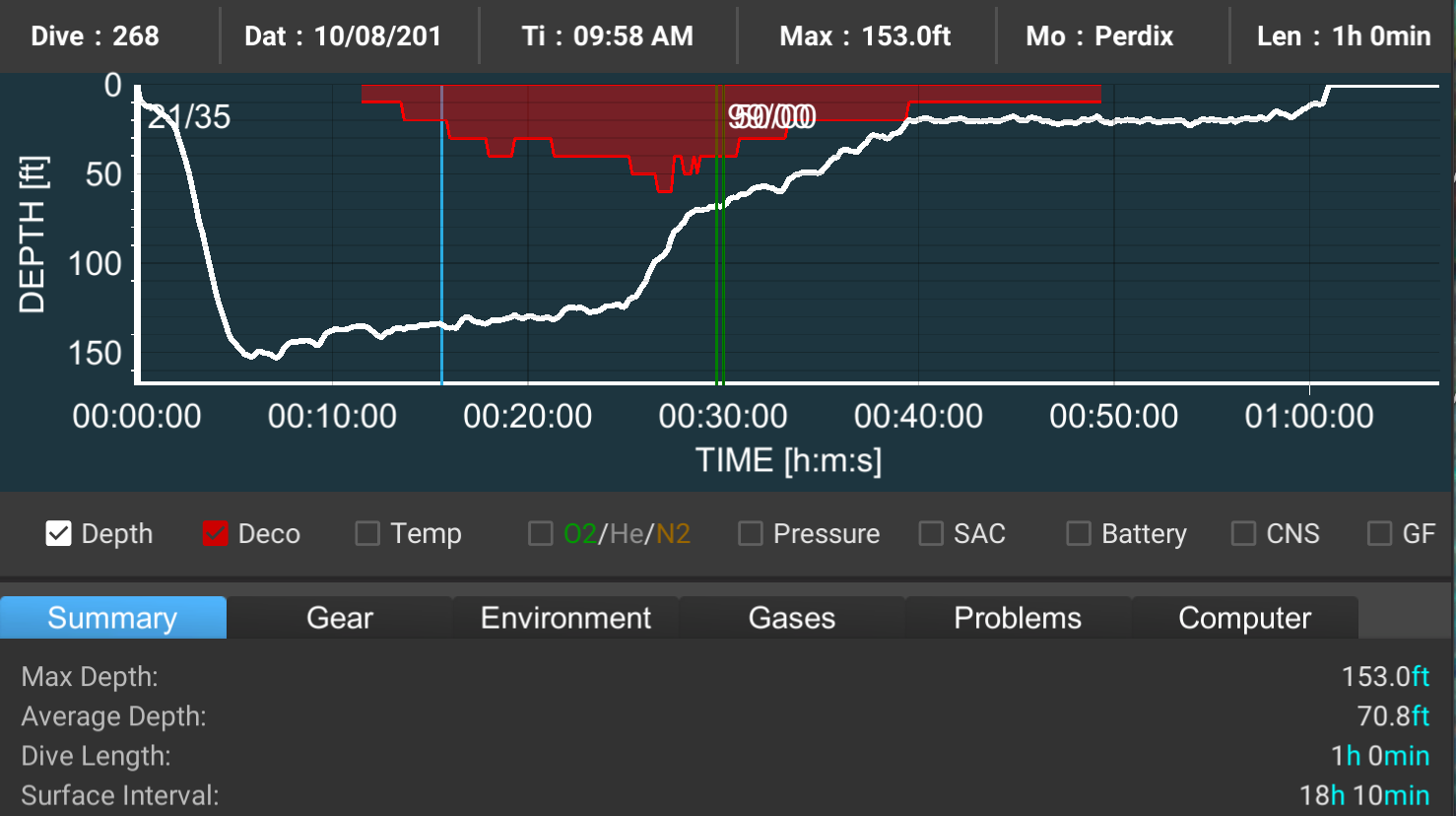
On day three we planned to dive to 150 ft/46 m on trimix 21/35 (21% oxygen, 35% helium), with 25 min bottom time with a gas switch to nitrox 50 at 70 ft/21 m. Our decompression profile used GUE modified deco based on Deco Planner with 2 min stops from 70 ft/21 m to 30 ft/10 m and a 16 min stop at 20 ft/6 m. The total planned run time for that dive was 58 min. At the start of our ascent, our average depth was only 132 ft/40 m, as we had worked our way slowly up the reef after hitting a max depth of 152 ft/46 m.




After a three-and-a-half-hour surface interval, we planned a 100 ft/30 m dive on nitrox 32 with a bottom time of 40 min with a gas switch to 100% O2 at 20 tf/6 m for 10 minutes for added conservativism. Total run time for that dive was 69 min, as we extended our 20 ft/6 m stop a lot longer to just hang and enjoy the reef.


Roughly two hours after this dive, Deana complained of itchy stinging skin on her hips and abdomen; she described it as being like stinging nettles. She was not concerned as this felt like what she had in Egypt, so we put her on 100% O2 for about an hour and a half and all symptoms resolved. Deana and I considered this a minor issue, and we did not talk to anyone about the symptoms since they quickly resolved. No further issues were experienced that evening.
It is here that human factors really played into the scenario. Deana and I made the mistake of not talking about the issue we had just experienced. We found out later the next day that Dr. Douglas Ebersole (cardiologist and consultant to Divers Alert Network) and the late Dr. Fiona Sharp (diving physician and anesthetist) were active participants of Buddy Dive Tek week. If we had spoken up, we most likely would have been able to talk to one or both of them and potentially decide not to dive the next morning. However, hindsight is 20/20, and we just didn’t feel the need to talk about it since Deana’s symptoms had been resolved.

The next morning Deana felt fine and showed no rash or issues from the previous day. She wanted to do the planned trimix dive to 150 ft. It was the same profile as the previous day’s dive, and the dive went without issue. We had completed an 18-hour surface interval, and Deco Planner showed we could dive the same profile with no additional decompression obligation.

About 45 min to an hour post dive, Deana complained of similar skin pain and stinging, but this time it extended down her thighs. When we returned to shore, we shared her symptoms with the technical diving supervisor, Mr. G, and placed her back on medical O2 for about two hours. This resolved the stinging, but Deana showed edema in her thighs, hips, and abdomen and deeper tissue pain. She had resolved to sit by the pool and have a Corona while I took a nap beside her to see if it would resolve itself.
We Called DAN
About an hour later Deana said, “We have DAN insurance, maybe we should call them and get their advice.” She placed a call to DAN, and within minutes was talking to Dr. Matías Nochetto. After a thorough assessment, Dr. Nochetto stated that, while they cannot diagnose over the phone, there were enough signs and symptoms to recommend we go into the ER and be assessed for DCI. DAN said that Bonaire had a hyperbaric chamber with an excellent team, and they gave us contact information for some of their team members. I cannot say enough good things about how DAN took so much worry away, offered a wealth of knowledge, and confirmed the direction we should take.
We followed DAN’s advice and told Mr. G what the plan was. Mr. G told us that Dr. Douglas Ebersole was one of the guest speakers and an active diver, and he located him for us before we went to the ER. Dr. Ebersole performed a neurological assessment in the parking lot and talked to Deana about her symptoms. He concurred that she needed to be assessed at the ER, and he felt she was showing signs of lymphatic DCI; his opinion gave us peace of mind, that while her condition wasn’t critical, it should still be checked at the ER.
After listening to Deana’s diving history over the last few years, he suggested undergoing a Transthoracic Echo (TTE) bubble study to rule out a Patent Forum Ovale (PFO), as this could explain her susceptibility to DCI. PFOs exist in almost a third of the population; although the condition isn’t rare, the condition can be activated due to the pressures exerted on our bodies at depth.
I drove Deana to the Bonaire ER, where the nursing team did a thorough assessment and showed great care, humor, and understanding. The ER nurse who took initial care of Deana was also a paramedic and technical diver and was wonderful to work with. After a full assessment, the ER doctor, who was not a diver, suggested that Deana made a poor choice in deciding to continue diving after a possible bout of skin bends. Deana later mentioned this comment to the ER nurse, adding that the doctor was not a diver and so likely didn’t understand. The ER nurse just smiled and agreed with her.

We were then visited by one of the hyperbaric physicians, who completed Deana’s neurological exam, which showed no signs of neurological DCI. He diagnosed her with DCI of the lymphatic system and said that recompression would be necessary to treat her symptoms. He gave her a saline IV and a Table 5 treatment in the chamber.
Deana did her 2.5 hour run in the chamber and did not notice any improvement in the pain or edema. However, her doctor told us that the pain and swelling of lymphatic DCI does not go away right after a chamber ride like with other types of DCI; DAN confirmed this when they followed up with us the next morning. We were told that the edema could take a few weeks to normalize. By the next day the pain had decreased, and Deana felt she was recovering. She did not dive any more on this trip, but still had a happy, positive demeanor, and she was the life of the party: Everyone wanted to know all about her chamber ride and experience.
Without undermining the risks associated with DCI, I want to mention the general positive outcome of this experience: we learned a great deal about Type 1 DCI, no one at our resort made Deana feel like she did something wrong, and everyone offered their support and understanding.

In Search of a PFO
In closing, I want to offer clarity on some frequent inquiries we’ve received about this story. Some suspected that dehydration may have played a part, but as an RN, Deana had more than doubled her water intake and was always staying hydrated. While dehydration can be a contributing factor to DCI, we do not feel that it was an issue in this case. People also asked about her alcohol intake. By the time of her second DCI hit that required recompression, she had had three Coronas and one mixed drink in three days. Her alcohol consumption was not an issue.

After coming back to the United States, Deana saw Dr. James Holm, who is one of the leading hyperbaric physicians at Virginia Mason in Seattle, and was highly recommended by DAN. Dr. Holm did a follow up examination and agreed that, based on her history, dive profiles, and the lymphatic DCI experience, Deana should get a TTE bubble study to check for a PFO. Deana scheduled a TTE through Overlake Hospital’s Advanced Cardiac Imagery Department. The results revealed that she does, in fact, have a mild-to-moderate PFO.

This diagnosis was bittersweet, as it explained why Deana had frequent incidents of DCI while diving within limits, but it now puts Deana in a position to weigh the risks and determine her next course of action. Both Dr. Holms and Dr. Aviles, an interventional cardiologist who diagnosed the PFO, did not recommend rushing into a PFO repair, which they said was not a silver bullet that would guarantee a DCI-free future.
Both physicians offered several suggestions for Deana to consider:
1. Stop diving, as this eliminates any risk of DCI in the future. For Deana this is not an option.
2. Modify her dive profile to be more conservative: diving only once per day, diving nitrox 32 but basing her profiles as if she was diving air, and/or extending her decompression profiles and safety stops.
3. Have the PFO repaired, knowing it is not a guarantee, and continue diving being as conservative as possible.
Dr. Aviles did say that if Deana plans on continuing the frequency and type of diving she has been currently doing, getting the PFO repaired is probably her best option. These are all choices that divers who have been diagnosed with a PFO have to wrestle with, and there is no right or wrong answer. While Deana is considering her options, she will look to be more conservative with her dives.
Like all types of higher risk sports, divers choose to accept the risk of being injured. For most divers, this is an acceptable risk, so we can enjoy the experiences we so cherish in exploring our aquatic environment. As divers we need to continually educate ourselves so we can make well-informed decisions that attempt to lower our risk of being injured.
Deana and I highly recommend Gareth Lock’s work on human factors for understanding how our decisions play into potential diving accidents. However, even with research and advancements in technology at our disposal, we still don’t understand DCI. There is no guarantee, even if we follow all the rules, that we will not get bent unless, of course, we stop diving. It is a risk we all take when we submerge beneath the water.
We have been amazed by the number of people we have met who discovered that they had a PFO in a way similar to Deana. Many have chosen to have their PFO corrected, though some have not, but all of them have been willing to share their experiences with us, helping us make a more informed decision. Next time you or a teammate shows any signs of DCI, tell someone and have it checked out. Sharing our experiences makes us safer, more educated divers.

For Part two of Deana’s story see: Undergoing PFO Surgery as a Team: Deana & Bert’s Excellent Adventure
Dive Deeper:
InDEPTH: Undergoing PFO Surgery as a Team: Deana & Bert’s Excellent Adventureby James D. Fraser
Gareth Lock, The Bend is Uninteresting…The Related Decisions Are Much More So

James D. Fraser is a PADI MSDT and NAUI Scuba Instructor and has been diving in the Pacific Northwest for over 30 years. James currently lives in Seattle, WA, with his wife and dive teammate Deana Fraser. Both James and Deana work at growing the local diving community and sharing their passion with all who are interested. James recently embraced technical diving, becoming certified as a Technical 1 diver with Global Underwater Explorers. James and Deana have had opportunities to travel all over the world to experience their passion in amazing places such as Egypt and the Maldives. James currently works as a Cyber Security Director with a Fortune 500 Defense Contractor and has been a residential construction business owner as an Emergency Medical Technician (EMT). James wants to expand his knowledge in the diving field and grow his experience in technical diving.























From Fear to Fieldwork: How Science Rewrites the Shark Story

“Deeper” with Dr. Richard Harris: A Movie Review

By Divers, For Divers: The iQsub CCR Story

Beneath the Jungle: The Connection That Changes Everything

North, South, and Nowhere Warm

Spinal DCS: A Personal and Professional View

