Community
Incident Report: Denial Isn’t Just a River in Egypt
As counter-errorism expert Gareth Lock, principal of Human in The System, explains: the river of denial runs deep through the diving community as demonstrated by this actual DCS incident. His report may help you find safe passage.
By Gareth Lock
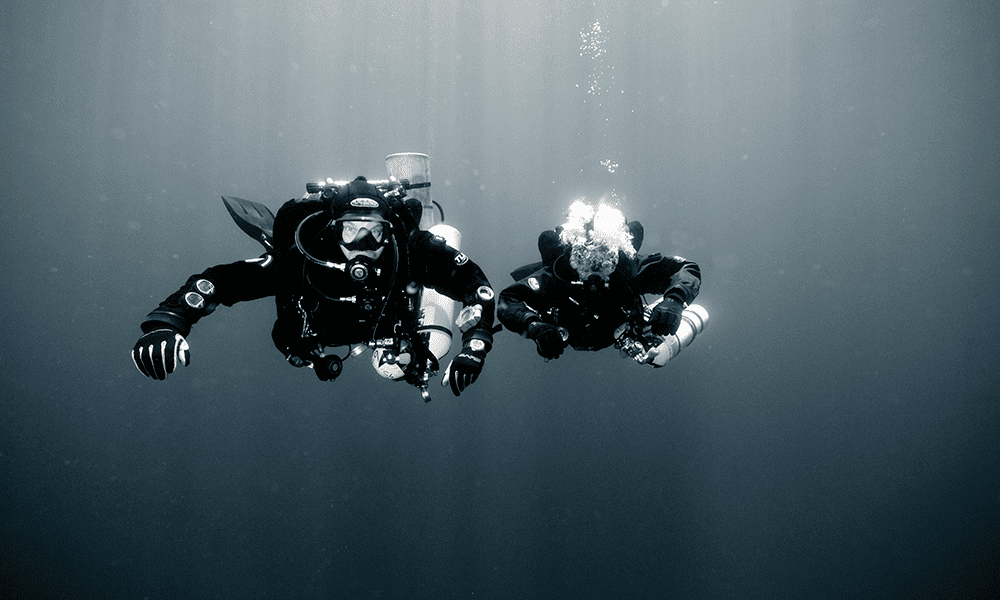
A pair of divers was completing their final dive following a week of 60-70 m/197-230 ft trimix diving off Malta in the Mediterranean Sea. The week had been brilliant. Blue skies, calm seas, and some amazing wrecks from the World War II era. This final dive was to be on the Italian fast patrol/torpedo boat Schnellboot S-31. It lays at 63 m/207 ft, almost intact and upright but broken in the middle, looking like someone had partially snapped it, like a stick.
They were planning on a 30-minute bottom time on open circuit using trimix 15/55, and nitrox 50% and 100% breathing gases. The dive itself was uneventful with some brilliant opportunities for photos in the clear water, and the decompression was completed as planned.
The interesting part started when one of the divers got back on the boat. As he took off his twinset, he noticed some disturbances in his vision. He had never had a migraine before, but it appears. in hindsight, to have been the same as the aura that those who suffer from migraines get. Even though the disturbances were obvious, the diver didn’t say anything to his buddy or others on the boat because they didn’t perceive any neurological or musculoskeletal signs or symptoms. After 20 minutes or so, while they were on their way back to the quayside, the visual disturbances cleared.
Approximately 30 minutes after surfacing, the boat arrived back at the quayside and the divers started to unload their equipment. There were multiple twinsets and stages to lift from the boat to the quayside and from the quayside onto the back of the flatbed trucks.















As the diver lifted the final twinset up onto the back of the flatbed, he immediately had a large “burst of light,” and his vision was disturbed. The disturbance was like an out-of-focus area moving across his vision, which meant that he couldn’t see clearly, especially in the focal area of vision. In the past, the diver had researched diving medical issues like PFOs and the link to DCS, and that physical exertion can open a patent foramen ovale (PFO) thereby allowing bubbles to cross from the venous side to the arterial side, which can lead to decompression sickness. At this point, the diver said to himself “I have a PFO!” However, he didn’t articulate this to the others in the team, again because there were no other signs/symptoms present. In his mind, he couldn’t detect any signs/symptoms of DCS, so it couldn’t be DCS!
The diver finished up moving the rest of the lighter equipment onto the flatbed and set off back to the dive center. He was unusually quiet, but no one mentioned anything to this effect. After 30-40 minutes, the visual disturbances cleared up. The diver still hadn’t said anything to anyone else at this stage, and there were still no signs or symptoms of DCS.
The following day the diver, his teammate, and the diver’s girlfriend flew back to the UK.
What are your thoughts on what happened? What do you think of the diver who didn’t declare his medical issue? Do your thoughts change if I said that diver was me?!
Most people have a negative thought process about the incident diver. If you fall into that category, you are likely to have one of the strongest biases people exhibit. It’s called a “fundamental attribution error.”
Most people have a negative thought process about the incident diver. If you fall into that category, you are likely to have one of the strongest biases people exhibit. It’s called a “fundamental attribution error.” This error can be summarized as: when a negative behavior is observed in someone else, we blame the individual, but when the same negative behavior is demonstrated by ourselves, then we attribute it to external factors. The Fundamental Attribution Error is one of the greatest barriers to learning when it comes to incidents and accidents because we don’t look at why it made sense for someone to do what they did. Lewin’s equation shows that our behaviour is a function of the person and the environment they are operating in. B=f(p,E). So before you judge, look at why it might have made sense for the person to do what they did. Local rationality is why something can appear irrational to someone on the outside, and yet make sense to the individual “inside”.
So what happened to me and why?
This was the last dive of a week’s great diving. My girlfriend (now wife) was holidaying with me in Malta while Howard (my teammate) and I went trimix diving. Kate doesn’t dive and was happy doing touristy stuff around the island while we dived.
I didn’t say anything to anyone on the quayside because I had a pretty good idea that if I did, I would be in a chamber and that would worry Kate; it would also mean we wouldn’t be flying back home the following day either, and I didn’t want to make a mess of the plans! In hindsight, it could have been a lot worse than it turned out. Irrational in hindsight. Locally rational if you think about what was going on in my head.
Upon my return to the UK, my tech instructor recommended a cardiologist who specializes in PFO treatments. I explained my circumstances to the doctor and told him that the dive had a conservative profile, explaining the gases and stops. He responded that “tech divers are a bunch of (expletive deleted) guinea pigs,” and upon reflection, I agreed. As a naval diving doctor now involved in commercial dive medicine, he advocates for more control and oversight than is current practice. He does not agree with tech divers taking the risks they do. The only way to confirm that I had a PFO was with a test.

Within two weeks, I had a transthoracic echocardiogram (TTE) whereby bubbles and saline were injected into a major vein in my left arm as my heart was imaged with ultrasound. At a specific point I was told to do a Valsalva maneuver to observe if bubbles would cross the heart. No bubbles were seen to cross the area where a PFO would be during any of the three times I complied. However, when I did a massive “sniff” as the bubbles were injected, immediately a shower of bubbles was seen crossing my heart wall through the PFO. Post-test analysis showed that I had an 8 mm x 12 mm PFO. You can see a video of my test here. (See attached video in the email).
Three months later I was in the operating theatre having the PFO fixed with an Amplatzer device. This is best described as two folded-up umbrellas inserted into the heart; the first is deployed on the inside of the heart, the second on the outside, and then as tension is applied, the two umbrellas close together pulling in the flap and closing the hole. Three months after that, I was back to diving, having been signed off as having no bubbles passing across the PFO. Prior to that event, I had had no signs or symptoms of DCS or anything linked with a PFO despite having completed approximately 400 dives and approximately 15 advanced trimix dives to 60-70 m/197-230 ft.
Summary
Denial is a massive issue in diving incidents, especially when it comes to DCS. I have seen numerous incident reports where the one managing the event is the last person who should be involved in the critical decision-making process! In 1993, Michael Menduno published an excellent article in aquaCORPS #5, BENT, which looked at the stigma associated with DCS. You can find it here.
Because of this stigma, the true prevalence of DCS is not really known and therefore the biases that we use to determine the likelihood of a risk materializing lack the data to inform them. Speaking to experts in the field, the real number of DCS events is likely to be four to eight times the reported level. Consequently, we need to change the attitude toward DCS as Jennifer Hunt’s article in aquaCORPS highlights.
There are numerous biases at play when we examine incidents, accidents, and near-hits. The most powerful of these are hindsight bias (where we “know” it would have happened that way) and the fundamental attribution error. In many cases, it is difficult to resist the effect of these biases, but being aware of them is the first step to improving learning throughout the diving community.
No one gets up in the morning and says “Today is a good day to get bent and not tell anyone anything about it.” We are doing the best we can with the resources we have and the pressures and drivers we are subject to. As Sir Andrew Hidden QC said when discussing the 1988 Clapham Junction train crash in which 35 people were killed and 484 were injured, “There is almost no human action or decision that cannot be made to look flawed and less sensible in the misleading light of hindsight. It is essential that the critic should himself be constantly aware of the fact.”
Like incident reports? Read another.

Gareth Lock has been involved in high-risk work since 1989. He spent 25 years in the Royal Air Force in a variety of front-line operational, research and development, and systems engineering roles which have given him a unique perspective. In 2005, he started his dive training with GUE and is now an advanced trimix diver (Tech 2) and JJ-CCR Normoxic trimix diver. In 2016, he formed The Human Diver with the goal of bringing his operational, human factors, and systems thinking to diving safety. Since then, he has trained more than 450 people face-to-face around the globe, taught nearly 2,000 people via online programmes, sold more than 4,000 copies of his book Under Pressure: Diving Deeper with Human Factors, and produced “If Only…,” a documentary about a fatal dive told through the lens of Human Factors and A Just Culture.























From Fear to Fieldwork: How Science Rewrites the Shark Story

By Divers, For Divers: The iQsub CCR Story

North, South, and Nowhere Warm

Spinal DCS: A Personal and Professional View

Technical Diving: Honoring the Man Behind the Name

Cave Biology: What Lives When Light Ends
