Diving Medicine
Cardiac Health Surveillance for Divers
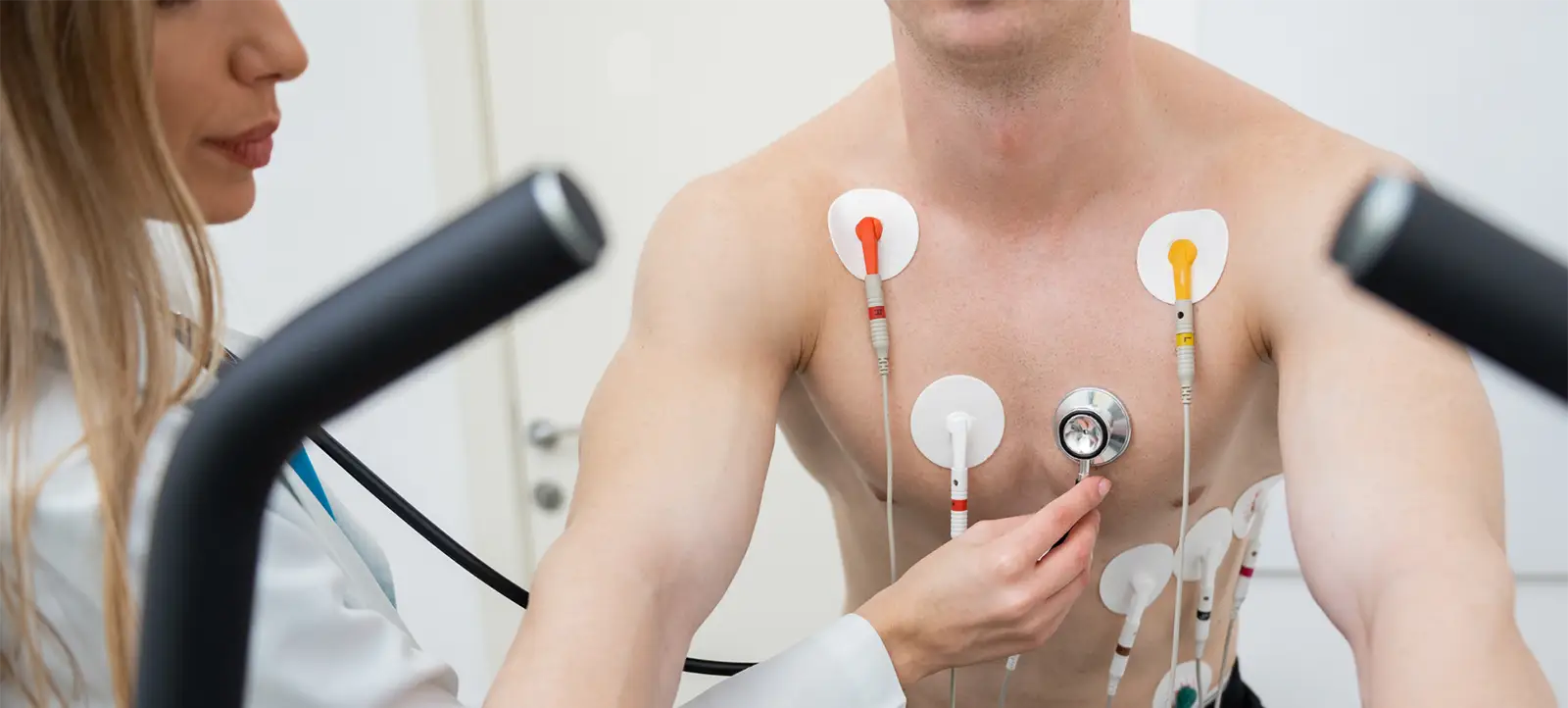
by Douglas Ebersole, MD. Photos courtesy of Watson Clinic, Lakland, FL.
Surprisingly, the proposal that rebreather divers 45-years and up have an annual cardiac health evaluation was one of the most hotly debated consensus statements at Rebreather Forum 4!?! Never mind that cardiovascular disease is the number one killer in the Western world, and second leading cause of diving deaths behind drowning! Here cardiologist and rebreather instructor Dr. Douglas Ebersole explains why cardiac health is so important, identifies the many risk factors, discusses fitness levels, cardiac testing protocols, and offers practical suggestions to help divers manage their risk.
Despite the advances in medicine over the past several decades, cardiovascular disease is still the number one killer in the Western world. There are over 16 million Americans with cardiovascular disease and, contrary to the usual perception, the number of men only slightly outnumbers women. Unfortunately, the first presentation of the disease is often a heart attack or sudden cardiac death.
Approximately 1.2 million of us will suffer a heart attack each year and 300,000 will die before reaching medical attention. Scuba divers are not immune to this disease. In the 2019 Divers Alert Network (DAN) Annual Diving Report, 15 of the 30 witnessed scuba diving deaths fit the description of sudden cardiac death while in 10 of 20 deaths with autopsy data, sudden cardiac death was the likely cause of the fatality.

Who Is At Risk?
The number one risk factor for the development of cardiovascular disease is simply advancing age. Even if you are young, remember you hope to be an “old” scuba diver one day. Hypertension, another strong risk factor, affects approximately 50 million Americans. Known as the “silent killer,” about one-third of those affected do not even know they have it. It, too, increases with advancing age. Around 50% of people over the age of 50 are hypertensive.
Another strong risk factor is diabetes mellitus. This endocrine disorder of glucose metabolism is strongly associated with obesity. With 30% of Americans being considered obese (body mass index greater than 30), it is not surprising that there is now a growing epidemic of diabetes in our country. Again, while some diabetics develop symptoms that aid in making the diagnosis, many only discover they have the disease on routine lab work ordered by their physician.





High cholesterol is another significant risk factor for the development of cardiovascular disease. It is also completely asymptomatic until the very late stages of the disease. Each of us should try to eat a low cholesterol, low fat diet. If this alone is not effective in reducing cholesterol numbers, there are a variety of medications to help. The goal for the general population should be a total cholesterol of < 200 mg/dL and an LDL of < 130 mg/dL. Anyone whose cholesterol is higher should first try diet and exercise. Most people with moderate to high cholesterol that is difficult to manage, should consider medication therapy.
A final “modifiable” risk factor is smoking. Despite the surgeon general’s warning about the hazards of tobacco use starting in 1969, as well as all the subsequent damning evidence that cigarette smoking drastically increases mortality rates, approximately 12% of adult Americans still smoke. While this is much lower than some other countries, it is concerning. Smoking is antithetical to diving, adversely affecting both heart and lungs, and at least one training agency, Global Underwater Explorers (GUE), will not train avowed smokers.
For all of these reasons, routine follow up (at least annually) with your primary physician is strongly recommended for all adults regardless of age.

What About Divers?
What does all of this have to do with diving? Well, there are growing numbers of older divers compared to a few decades ago. These divers are at significant risk of cardiovascular disease. The reason for this is two-fold. First, many of us who started diving several decades ago as younger and fitter versions of ourselves are now over 50 with increased waistlines and decreased fitness levels. Secondly, as dive equipment has improved and become more reliable through the years, more older divers have entered our sport.
While some divers prefer to think that the statistics don’t apply to them, that in fact scuba diving renders them immune to the perils of aging, the numbers from Divers Alert Network (DAN) prove otherwise. Of the 80-90 deaths among US and Canadian divers annually cited in DAN’s 2019 Annual Diving Report, cardiovascular disease is the second leading cause of death behind drowning. Additionally, 80% of these deaths occurred in those 40 years or older with hypertension and cardiovascular disease as the most common preceding medical conditions.
Of the 80-90 deaths among US and Canadian divers annually, cardiovascular disease is the second leading cause of death behind drowning. Additionally, 80% of these deaths occurred in those 40 years or older with hypertension and cardiovascular disease as the most common preceding medical conditions.

Problems arise when the heart’s demand for blood exceeds its supply. As we all know, the heart pumps blood to the whole body. It must also pump blood to itself. It does this through the coronary arteries. These vessels arise from the proximal aorta and are the first branches that arise after blood exits the heart. These three coronary arteries course along the surface of the heart with sub-branches that dive into the heart muscle.
Cholesterol buildup in these vessels limits blood flow. The importance of this buildup depends on the location and severity of the blockage limiting blood supply to the heart as well as the demand for blood by the heart which depends on the heart’s workload.
In general, workloads involved in scuba diving are not that high, but these workloads can change dramatically due to conditions: currents, rough seas, distance to the dive site carrying equipment, and other extenuating circumstances. Additionally, just being submerged in water–especially cold water–increases stress on the heart as blood is shunted from the extremities to the central circulation. This results in an estimated average 700 mL arterial blood shift.
There is also reduced lung compliance when submerged, increasing the work of breathing. The cooling effect of the water results in vasoconstriction and increased blood pressure. Also, in a water environment, divers don’t get the usual “hot and sweaty” sensation when they are working hard that they are used to on land. Finally, with diving, they may not be able to simply stop the activity if symptoms develop, as they could do when engaged in most physical activities.

What Kind Of Fitness Should One Have For Scuba Diving?
The answer to this question requires a little bit of physiology. The first concept is that of oxygen consumption. At rest, our bodies consume approximately 3.5 mL/kg/min of oxygen, which is defined as one metabolic equivalent (MET). While we all have about this same minimal oxygen consumption, maximal oxygen consumption varies dramatically among individuals. Depending on one’s fitness level, a diver will have a different maximum oxygen consumption compared to his buddy. At or below 50% of this maximum value, a person can sustain work for a prolonged time.
Swimming at a speed of one knot requires 28 mL/kg/min or about 8 MET. Most diving is well below this, but these conditions could arise if you need to swim against a moderate current. In general, recreational scuba divers should be able to walk two miles/3.2 km in under 30 minutes, as this would be a sustained workload of 6.5 METs, or about the workload of swimming at one knot as above. Cardiac stress testing is a good way to assess both aerobic fitness and the likelihood of significant coronary artery disease in the diver.




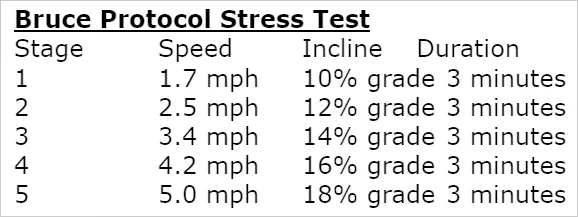
If divers can complete Stage 2 of a Bruce Protocol (six minutes total), they are fit enough for recreational scuba diving. Dive professionals and technical divers should have a greater degree of fitness and should be able to complete at least Stage 3 of a Bruce Protocol (nine minutes total). It is also recommended that individuals older than 40 years should undergo risk assessment for coronary artery disease. Stress testing can be helpful in this regard as well. Please note that you primary physician or cardiologist can order a stress test for you.
Bruce Protocol Stress Test
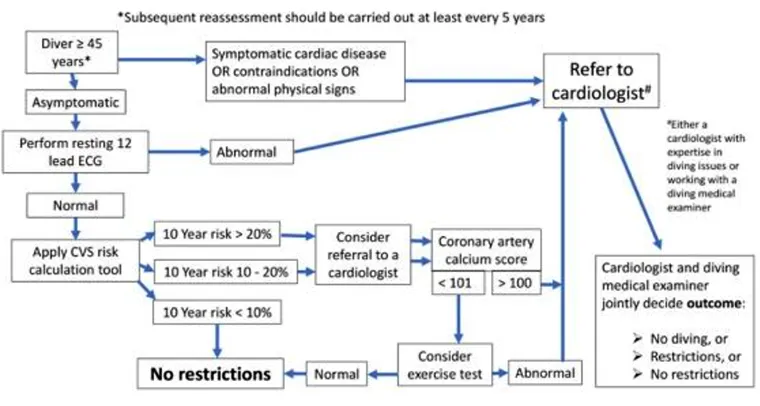
Below is a recommended flow chart for all divers aged 45 years and older from the South Pacific Underwater Medical Society published in Diving and Hyperbaric Medicine (Jepsen N. et al. South Pacific Underwater Medicine Society guidelines for cardiovascular risk assessment of divers. Diving Hyperb Med. 2020;50(3):273-277). It suggests initially using an electrocardiogram (ECG), and cardiovascular risk assessment to stratify divers.
Here is a link to a 10-year Cardiovascular Risk Assessment tool: Calculator: Cardiovascular risk assessment in adults
I’ve Developed Heart Disease. Now What?
What about divers who have cardiovascular disease? Yes, it is possible to dive after having a heart attack, coronary stenting, and/or bypass surgery. After recovering from the event and being cleared by your physician, you can return to diving. You simply need to have normal heart muscle function which can be assessed with ultrasound imaging (echocardiogram), good exercise tolerance as outlined above, and no evidence of ischemia (limitation of blood flow to the heart) on stress testing.






What About Drugs?
After the development of coronary artery disease, most patients will go home on a combination of blood thinners, cholesterol lowering medications, and possibly beta blockers and/or angiotensin converting enzyme (ACE) inhibitors. While drugs such as aspirin and clopidogrel (Plavix) do slightly increase a diver’s risk of bleeding, they can safely be taken while diving. The same holds true for beta blockers. Please note however, that beta blockers can limit exercise ability and should be evaluated with exercise testing. As with all medications, the effects of these drugs in the hyperbaric conditions of scuba diving are unclear. It is generally recommended that you take any new medication for several weeks before diving so that you can see how it affects you.

Last Line Of Defense
In conclusion, cardiovascular disease is extremely prevalent in our society and the leading cause of death in the western world. There are certain risk factors such as advancing age that we cannot change, but others such as hypertension, diabetes mellitus, hypercholesterolemia, and smoking that are modifiable. Unfortunately, hypertension, diabetes, and hypercholesterolemia are often completely asymptomatic and may only be found during a medical evaluation.
While we should all strive to control these risk factors by avoiding tobacco use, eating a healthy diet, and exercising regularly, we should also make sure we have regular follow up with our primary physician. Above is a recommended flow chart every diver should follow at least every five years.
Finally, it is important to note that, if despite your best efforts, you develop cardiovascular disease, it is not necessarily the end of your diving career. With current medications and therapies, there is hope that we can all enjoy this sport well into our “golden years.”
DIVE DEEPER
Alert Diver: Medical Examination of Diving Fatalities. Proceedings Summary | DAN and UHMS Medical Examination of Diving Fatalities Symposium
DHM: South Pacific Underwater Medicine Society guidelines for cardiovascular risk assessment of divers by Jepson N, Rienks R, Smart D, Bennett MH, Mitchell SJ, Turner M.
InDEPTH: Everything You wanted To Know About PFOs and Decompression Illness, But Were Too Busy Decompressing to Ask by Dr. Douglas Ebersole
InDEPTH: RF4 Consensus Statements by Drs. Simon J. Mitchell and Neal W. Pollock. The citation for the formally published paper is here: Mitchell SJ, Pollock NW. Rebreather Forum Four consensus statements. Diving Hyperb Med. 2023 June 30; 53(2): 142-146
RF4 Consensus Statements: Cardiac Health Surveillance
The forum endorses the principle of periodic cardiac health surveillance for all rebreather divers with an emphasis on targeted annual or biennial evaluation for divers older than 45 years even in apparent good health.

Dr. Douglas Ebersole, MD, is a cardiologist specializing in coronary and structural heart interventions at the Watson Clinic LLP in Lakeland, Florida, and a cardiology consultant to Divers Alert network (DAN). He is also an avid technical, cave, and rebreather diver and instructor. He can be reached at [email protected].

























Los Factores de Gradiente en un Mundo Posterior a las Paradas Profundas

Can You Really Make Diving a Day Job? The Realities of Full-Time Tech Instruction
Deco Dilemmas: The Push for Personalized Decompression Modeling

An Analysis of Cave Diving Accidents

What Not To Die For: A Guide to Efficient Expenditure of Human Resources

The State of Personalized Decompression
